
HCA 54-0021 (8/23)
Printed under the direction of the Washington State Health Care Authority Public Employees Benets Board (PEBB)
Self-insured by the State of Washington · Eective January 1, 2024
2024 UMP Consumer-Directed Health Plan (PEBB)
Certicate of Coverage
2024 UMP CDHP (PEBB) Certificate of Coverage
2024 UMP CDHP (PEBB) Certificate of Coverage 1
Directory
Directory: medical services
Contact type and description
Contact information
UMP Customer Service
Contact UMP Customer Service
for questions about your medical
benefits, including information
on behavioral health support
services, the expert second
opinion program, your care
management benefit, and more.
Call: 1-888-849-3681 (TRS: 711)
Monday–Friday: 5 a.m. to 8 p.m.; Saturday: 8 a.m. to 4:30 p.m.
(Pacific)
Chat now: Sign in to your Regence account at
ump.regence.com/ump/signin to chat now
Monday–Friday: 5 a.m. to 8 p.m.; Saturday: 8 a.m. to 4:30 p.m.
Email: Send secure email via your Regence account at
ump.regence.com/ump/signin
Visit: UMP website at ump.regence.com/pebb
If you are outside the U.S. and you have questions about your
benefits and coverage, you can use email, chat now, or Skype to
contact UMP Customer Service. You may request to have a
customer service representative contact you at a scheduled time
during normal business hours.
If you are outside the U.S. and need to find a local provider, make
an appointment, or be hospitalized, call Blue Cross Blue Shield
Global® Core at 1-800-810-2583 or call collect at 1-804-673-1177,
24 hours a day, 7 days a week. You can also use the online provider
search tool on the Blue Cross Blue Shield Global Core website at
bcbsglobalcore.com.
Network provider directory
Call: 1-888-849-3681 (TRS: 711)
Monday–Friday: 5 a.m. to 8 p.m.; Saturday: 8 a.m. to 4:30 p.m.
(Pacific)
Chat now: Sign in to your Regence account at
ump.regence.com/ump/signin to chat now
Monday–Friday: 5 a.m. to 8 p.m.; Saturday: 8 a.m. to 4:30 p.m.
(Pacific)
Provider search: ump.regence.com/go/pebb/UMP-CDHP
Medical appeals and grievances
(aka complaints)
Call: 1-888-849-3681 (TRS: 711)
Monday–Friday: 5 a.m. to 8 p.m.; Saturday: 8 a.m. to 4:30 p.m.
(Pacific)
Chat now: Sign in to your Regence account at
ump.regence.com/ump/signin to chat now
Monday–Friday: 5 a.m. to 8 p.m.; Saturday: 8 a.m. to 4:30 p.m.
(Pacific)
Fax: 1-877-663-7526
Online: Sign in to your secure Regence account at
ump.regence.com/ump/signin. Go to Appeals to appeal online.
Email: UMPmemberappeals@regence.com
2 2024 UMP CDHP (PEBB) Certificate of Coverage
Contact type and description
Contact information
Mail:
UMP Appeals and Grievances
Regence BlueShield
PO Box 1106
Lewiston, ID 83501-1106
Preauthorization
For providers submitting medical
service preauthorization requests
Call: 1-888-849-3682 (TRS: 711)
Monday–Friday: 7 a.m. to 5 p.m. (Pacific)
Fax: 1-844-679-7763
Visit: availity.com
Access to medical claims
Visit: Sign in to your Regence account at
ump.regence.com/ump/signin
Claims
For members submitting medical
service claims
Fax: 1-877-357-3418
Mail:
Regence BlueShield
Attn: UMP Claims
PO Box 1106
Lewiston, ID 83501-1106
Coordination of benefits
Contact UMP if you or your
dependents have other insurance
to make sure your claims are
processed correctly. You may fax
or mail the “Multiple Coverage
Inquiry” form to UMP.
Call: 1-888-849-3681 (TRS: 711) to request a form
Visit: UMP commonly used forms available online webpage at
ump.regence.com/pebb/forms/common-forms and under
Medical forms choose the “Multiple Coverage Inquiry” form
Fax: 1-877-357-3418
Mail:
Regence BlueShield
Attn: UMP Claims
PO Box 1106
Lewiston, ID 83501-1106
HealthEquity
Health savings account (HSA)
trustee
Call: 1-844-351-6853 (TRS: 711), 24 hours, 7 days a week
Visit: HealthEquity website at learn.healthequity.com/pebb
Medicare
Call: 1-800-MEDICARE (1-800-633-4227) (TTY: 1-877-486-2048)
24 hours, 7 days a week
Visit: medicare.gov or MyMedicare.gov
Eligibility, enrollment, and
address changes
Employees: Contact your payroll or benefits office
Continuation Coverage and retired employees of a former
employer group: Call the PEBB Program: 1-800-200-1004 (TRS:
711)
Retirees: Call the PEBB Program: 1-800-200-1004 (TRS: 711)
Monday–Friday: 8 a.m. to 4:30 p.m. (Pacific)
Visit: hca.wa.gov/erb
2024 UMP CDHP (PEBB) Certificate of Coverage 3
Contact type and description
Contact information
Medical policies that affect
coverage or care
Including preauthorization,
Health Technology Clinical
Committee (HTCC) information,
clinical policies, and drugs
covered under medical benefits
Visit: Policies that affect your care webpage at
ump.regence.com/pebb/benefits/policies
4 2024 UMP CDHP (PEBB) Certificate of Coverage
Directory: vision services
Contact type and description
Contact information
UMP vision benefits
Get an overview of your vision
benefit
Visit: UMP Vison benefits webpage at
ump.regence.com/pebb/benefits/vision
Vision Service Plan (VSP)
Member Services
Call: 1-844-299-3041
Monday–Friday: 6 a.m. to 8 p.m.; Saturday: 7 a.m. to 8 p.m.; Sunday
8 a.m. to 8 p.m. (Pacific). If you are outside of the U.S. dial the exit
code of your country, which is typically 00, and then 1-916-635-
7373.
Deaf, DeafBlind, Late Deafened and Hard of Hearing
members call (TTY): 1-800-428-4833
Monday–Saturday: 6 a.m. to 5 p.m.; Sunday 5 a.m. to 8 p.m.
(Pacific). If you are outside of the U.S. dial the exit code of your
country, which is typically 00, and then 1-916-851-1375.
Visit: VSP website at vsp.com
Mail:
Vision Service Plan
PO Box 997100
Sacramento, CA 95899-7100
VSP provider directory
Provider search: Create an account on the VSP website at
vsp.com and log in to find a VSP Choice network provider. If you
don’t have an account, you can visit the VSP website at
vsp.com/eye-doctor, use the Advanced search, and select
“Choice” for the “Doctor network” to find a provider.
Call: 1-844-299-3041
Monday–Friday: 6 a.m. to 8 p.m.; Saturday: 7 a.m. to 8 p.m.; Sunday
8 a.m. to 8 p.m. (Pacific)
Deaf, DeafBlind, Late Deafened and Hard of Hearing members
call (TTY): 1-800-428-4833
Monday–Saturday: 6 a.m. to 5 p.m.; Sunday 5 a.m. to 8 p.m.
(Pacific)
VSP appeals
Call: 1-844-299-3041 to submit an expedited appeal (will be
processed within 24 hours)
Monday–Friday: 6 a.m. to 8 p.m.; Saturday: 7 a.m. to 8 p.m.; Sunday
8 a.m. to 8 p.m. (Pacific)
Deaf, DeafBlind, Late Deafened and Hard of Hearing
members call (TTY): 1-800-428-4833
Monday–Saturday: 6 a.m. to 5 p.m.; Sunday 5 a.m. to 8 p.m.
(Pacific)
Mail: To appeal in writing with VSP, including expedited appeals:
Vision Service Plan
Attn: Appeals Department
PO Box 2350
Rancho Cordova, CA 95741
2024 UMP CDHP (PEBB) Certificate of Coverage 5
Contact type and description
Contact information
VSP complaints
Call: 1-844-299-3041
Monday–Friday: 6 a.m. to 8 p.m.; Saturday: 7 a.m. to 8 p.m.; Sunday
8 a.m. to 8 p.m. (Pacific)
Deaf, DeafBlind, Late Deafened and Hard of Hearing members
call (TTY): 1-800-428-4833
Monday–Saturday: 6 a.m. to 5 p.m.; Sunday 5 a.m. to 8 p.m.
(Pacific)
Visit: VSP website at vsp.com/contact-us/grievance and complete
the online form.
Mail:
Vision Service Plan
Attention: Complaint and Grievance Unit
PO Box 997100
Sacramento, CA 95899-7100
VSP Claims
Call: 1-844-299-3041 to request a VSP Member Reimbursement
Form.
Monday–Friday: 6 a.m. to 8 p.m.; Saturday: 7 a.m. to 8 p.m.; Sunday
8 a.m. to 8 p.m. (Pacific)
(TTY): 1-800-428-4833 to request a VSP Member Reimbursement
Form. If you are outside of the U.S. and you need to submit a claim
form for services received outside the U.S. dial the exit code of
your country, which is typically 00, and then 1-916-851-1375.
Monday–Saturday: 6 a.m. to 5 p.m.; Sunday 5 a.m. to 8 p.m.
(Pacific)
Visit: VSP website at vsp.com/claims/submit-oon-claim and
select “Start new claim” to submit an out-of-network claim online
Mail:
Vision Service Plan
Attention: Claims Services
PO Box 495918
Cincinnati, OH 45249-5918
Directory: prescription drug services
Contact type and description
Contact information
Prescription drugs
Contact customer service, locate
network pharmacies, ask
prescription drug questions,
access your WSRxS account, and
check prescription drug prices
Washington State Rx Services (WSRxS)
Call: 1-888-361-1611 (TRS: 711)
Monday–Friday: 7:30 a.m. to 5:30 p.m. (Pacific)
Available outside these hours with limited services.
Visit: Prescription drug coverage webpage at
ump.regence.com/pebb/benefits/prescriptions
Network mail-order pharmacies
Costco Mail-Order Pharmacy
Deaf, DeafBlind, Late Deafened and Hard of Hearing members
6 2024 UMP CDHP (PEBB) Certificate of Coverage
Contact type and description
Contact information
Order new prescriptions and
refills, check order status, manage
prescriptions, track your package
UMP members do not need to be Costco members to use their
mail-order service.
Call: 1-800-607-6861 (TRS: 711)
Monday–Friday: 5 a.m. to 7 p.m.; Saturday: 9:30 a.m. to 2 p.m.
(Pacific)
Providers fax: 1-800-633-0334
Mailing a prescription order:
Costco Pharmacy (#581)
802 134th St SW STE 140
Everett, WA 98204-7314
Visit: Sign in to your Costco account at pharmacy.costco.com
Postal Prescription Services (PPS)
Call: 1-800-552-6694 (TRS: 711)
Monday–Friday: 6 a.m. to 6 p.m.; Saturday: 9:30 a.m. to 2 p.m.
(Pacific)
Providers fax: 1-800-723-9023
Mailing a prescription order:
Postal Prescription Services
PO Box 2718
Portland, OR 97208-2718
Visit: Sign in to your PPS account at ppsrx.com
Network specialty drug
pharmacy
Order new prescriptions and
refills for specialty drugs
Ardon Health
Call: 1-855-425-4085 (TRS: 711)
Monday–Friday: 8 a.m. to 7 p.m.; Saturday: 8 a.m. to 12 p.m.
(Pacific)
Closed Sundays and all major holidays
For urgent health questions that require the assistance of a
clinician after-hours, you can reach an Ardon Health pharmacist 24
hours a day, seven days a week, by calling 1-855-425-4085 and
following the prompts.
Providers fax: 1-855-425-4096
Visit: ardonhealth.com
Email: info@ardonhealth.com (This email is not secure)
Prescription drug appeals and
complaints
WSRxS
Call: 1-888-361-1611 (TRS: 711)
Monday–Friday: 7:30 a.m. to 5:30 p.m. (Pacific)
Fax appeals to: 1-866-923-0412
Mail:
WSRxS
Attn: Appeal Unit
PO Box 40168
Portland, OR 97240-0168

2024 UMP CDHP (PEBB) Certificate of Coverage 7
Contact type and description
Contact information
Prescription drug
preauthorization
For providers and pharmacists
submitting prescription drug
preauthorization requests,
including requests for an
exception for noncovered
prescription drugs or changing
quantity limits
WSRxS
Call: 1-888-361-1611 (TRS: 711)
Monday–Friday: 7:30 a.m. to 5:30 p.m. (Pacific)
Fax: 1-800-207-8235
Visit: covermymeds.com
Prescription drug claims
WSRxS
Call: 1-888-361-1611 (TRS: 711)
Monday–Friday: 7:30 a.m. to 5:30 p.m. (Pacific)
Fax: 1-855-668-8550
Mail:
Pharmacy Manual Claims
PO Box 999
Appleton, WI 54912-0999
Visit: Find claim forms by visiting forms and publications at
hca.wa.gov/ump-forms-pubs
Coordination of benefits
Contact WSRxS if you or your
dependents have other insurance
to make sure your claims are
processed correctly. You may fax,
email, or mail the “WSRxS
Multiple Prescription Drug
Coverage Inquiry” form to WSRxS.
WSRxS
Call: 1-888-361-1611 (TRS: 711) to request a form.
Visit: UMP commonly used forms available online webpage at
ump.regence.com/pebb/forms/common-forms and under
Prescription drug forms choose the “WSRxS Multiple Prescription
Drug Coverage Inquiry” form
Fax: 1-855-668-8550
Email: Send email through your WSRxS account at
ump.regence.com/pebb/benefits/prescriptions
(This email is not secure)
Mail:
Pharmacy Manual Claims
PO Box 999
Appleton, WI 54912-0999
8 2024 UMP CDHP (PEBB) Certificate of Coverage
Table of Contents
Directory .................................................................................................................................................................................................. 1
Directory: medical services ......................................................................................................................................................... 1
Directory: vision services ............................................................................................................................................................. 4
Directory: prescription drug services ..................................................................................................................................... 5
Online services ................................................................................................................................................................................... 13
How to use this certificate of coverage ................................................................................................................................. 14
About UMP CDHP ............................................................................................................................................................................ 14
Features of UMP CDHP ............................................................................................................................................................. 14
Accumulators ..................................................................................................................................................................................... 15
Finding a health care provider ................................................................................................................................................... 15
Sample payments to different provider network status ............................................................................................ 17
How to find a preferred provider ......................................................................................................................................... 18
Covered and noncovered provider types ......................................................................................................................... 19
Primary care providers .............................................................................................................................................................. 19
When you do not have access to a preferred provider: network waiver ........................................................... 19
When and how to request a network waiver .................................................................................................................. 20
How an HSA works...................................................................................................................................................................... 21
Out-of-area services ................................................................................................................................................................... 21
Services received outside the United States ................................................................................................................... 23
What you pay for services ............................................................................................................................................................ 25
Deductible ....................................................................................................................................................................................... 25
Coinsurance .................................................................................................................................................................................... 27
When you pay ............................................................................................................................................................................... 27
Health savings account (HSA) ................................................................................................................................................ 27
Out-of-pocket limit ..................................................................................................................................................................... 28
Summary of services and payments ........................................................................................................................................ 29
Deductible and limits ................................................................................................................................................................. 31
Types of services .......................................................................................................................................................................... 31
What else you need to know .................................................................................................................................................. 34
Benefits: what the plan covers ................................................................................................................................................... 34
Guidelines for coverage ............................................................................................................................................................ 34
Health Technology Clinical Committee (HTCC) ............................................................................................................. 35
Summary of benefits .................................................................................................................................................................. 36
List of benefits ............................................................................................................................................................................... 39
Acupuncture .............................................................................................................................................................................. 39
2024 UMP CDHP (PEBB) Certificate of Coverage 9
Ambulance ................................................................................................................................................................................. 39
Applied Behavior Analysis (ABA) Therapy ................................................................................................................... 40
Autism treatment .................................................................................................................................................................... 40
Bariatric surgery ....................................................................................................................................................................... 41
Behavioral health .................................................................................................................................................................... 41
Breast health screening tests ............................................................................................................................................. 44
Care Gap Closure Program ................................................................................................................................................. 44
Care management .................................................................................................................................................................. 44
Chiropractic physician services ......................................................................................................................................... 45
Dental services.......................................................................................................................................................................... 45
Diabetes care supplies .......................................................................................................................................................... 46
Diabetes Control Program .................................................................................................................................................. 47
Diabetes education ................................................................................................................................................................ 47
Diabetes Prevention Program (DPP) .............................................................................................................................. 47
Diagnostic tests, laboratory, and x-rays ....................................................................................................................... 48
Dialysis ......................................................................................................................................................................................... 48
Durable medical equipment (DME), supplies, and prostheses........................................................................... 48
Emergency room ..................................................................................................................................................................... 51
End-of-life counseling .......................................................................................................................................................... 51
Family planning services ...................................................................................................................................................... 51
Foot care, maintenance ........................................................................................................................................................ 52
Gender affirming care ........................................................................................................................................................... 52
Genetic services ....................................................................................................................................................................... 53
Headaches, chronic migraine or chronic tension type ........................................................................................... 53
Hearing care (diseases and disorders of the ear) ..................................................................................................... 53
Home health care .................................................................................................................................................................... 54
Hospice care .............................................................................................................................................................................. 55
Hospital services ...................................................................................................................................................................... 56
Infusion drug site of care program ................................................................................................................................. 57
Joint replacement surgery, knees and hips in the Centers of Excellence (COE) Program ..................... 58
Knee arthroplasty, total ........................................................................................................................................................ 60
Mammogram and Digital Breast Tomosynthesis (DBT) ........................................................................................ 61
Massage therapy ..................................................................................................................................................................... 61
Mastectomy and breast reconstruction ........................................................................................................................ 62
Mental health ............................................................................................................................................................................ 62
Naturopathic physician services ....................................................................................................................................... 62
Nurse line .................................................................................................................................................................................... 62
10 2024 UMP CDHP (PEBB) Certificate of Coverage
Nutrition counseling and therapy ................................................................................................................................... 62
Obstetric and newborn care ............................................................................................................................................... 63
Office visits ................................................................................................................................................................................. 65
Orthognathic and Telegnathic surgery ......................................................................................................................... 65
Pain and joint management, interventional ............................................................................................................... 65
Prescription drugs................................................................................................................................................................... 65
Preventive care ......................................................................................................................................................................... 65
Radiology .................................................................................................................................................................................... 68
Second opinions ...................................................................................................................................................................... 68
Skilled nursing facility ........................................................................................................................................................... 69
Sleep therapy ............................................................................................................................................................................ 69
Spinal and extremity manipulations............................................................................................................................... 70
Spinal injections ....................................................................................................................................................................... 70
Spinal surgery ........................................................................................................................................................................... 70
Spine care in the Centers of Excellence (COE) Program ........................................................................................ 70
Substance use disorder ........................................................................................................................................................ 73
Surgery ......................................................................................................................................................................................... 73
Temporomandibular joint (TMJ) disorder treatment ............................................................................................. 74
Therapy: Habilitative and Rehabilitative ...................................................................................................................... 74
Tobacco cessation services ................................................................................................................................................. 75
Transplants ................................................................................................................................................................................. 77
Urgent care ................................................................................................................................................................................ 77
Virtual care ................................................................................................................................................................................. 77
Vision care (diseases and disorders of the eye) ........................................................................................................ 79
Your routine vision benefits ........................................................................................................................................................ 79
Finding a routine vision provider ......................................................................................................................................... 79
Adults (age 19 or older) ............................................................................................................................................................ 80
Children (under age 19) ............................................................................................................................................................. 83
Vision claims administration .................................................................................................................................................. 85
Vision complaints and appeals .............................................................................................................................................. 86
Your prescription drug benefit .................................................................................................................................................. 87
The UMP Preferred Drug List ................................................................................................................................................. 87
How UMP decides which prescription drugs are preferred ..................................................................................... 89
Guidelines for prescription drugs UMP covers .............................................................................................................. 90
What you pay for prescription drugs ................................................................................................................................. 92
Where to buy your prescription drugs .............................................................................................................................. 94
Limits on your prescription drug coverage ..................................................................................................................... 97
2024 UMP CDHP (PEBB) Certificate of Coverage 11
What to do if the plan denies coverage .......................................................................................................................... 102
Prescription drugs and products UMP does not cover ............................................................................................ 102
Limits on plan coverage .............................................................................................................................................................. 103
Preauthorizing medical services ......................................................................................................................................... 103
General information from UMP Customer Service ..................................................................................................... 105
What the plan does not cover .................................................................................................................................................. 106
If you have other HDHP coverage .......................................................................................................................................... 116
Coordination of benefits ........................................................................................................................................................ 116
Contact UMP and WSRxS ....................................................................................................................................................... 117
Who pays first ............................................................................................................................................................................. 117
Billing and payment: submitting a claim ............................................................................................................................. 121
Submitting a claim for medical services.......................................................................................................................... 121
Submitting a claim for prescription drugs ..................................................................................................................... 123
False claims or statements ..................................................................................................................................................... 124
Complaint and appeal procedures ......................................................................................................................................... 124
What is a complaint (aka: grievance)? ............................................................................................................................. 124
How to submit a complaint (aka: grievance) ................................................................................................................ 125
What is an appeal? .................................................................................................................................................................... 125
The appeals process ................................................................................................................................................................. 125
Complaints about quality of care ....................................................................................................................................... 129
Appeals related to eligibility................................................................................................................................................. 130
Where to send complaints or appeals ............................................................................................................................. 130
When another party is responsible for injury or illness ................................................................................................ 130
Occupational injury or illness (workers’ compensation) claims ........................................................................... 130
Legal rights and responsibilities ......................................................................................................................................... 130
Fees and expenses ..................................................................................................................................................................... 132
Services covered by other insurance ................................................................................................................................ 132
Motor vehicle coverage .......................................................................................................................................................... 132
Future medical expenses ........................................................................................................................................................ 132
General provisions ......................................................................................................................................................................... 133
What you need to know: your rights and responsibilities ...................................................................................... 133
Relationship to Blue Cross and Blue Shield Association .......................................................................................... 137
Right to receive and release needed information ...................................................................................................... 137
Right of recovery ....................................................................................................................................................................... 137
Limitations on liability ............................................................................................................................................................. 137
Governing law ............................................................................................................................................................................. 137
Anti-assignment ......................................................................................................................................................................... 137
12 2024 UMP CDHP (PEBB) Certificate of Coverage
No waiver ...................................................................................................................................................................................... 138
Acronyms ........................................................................................................................................................................................... 139
Eligibility and enrollment ........................................................................................................................................................... 140
Eligibility for subscribers and dependents ..................................................................................................................... 140
Enrollment for subscribers and dependents ................................................................................................................. 141
Medicare eligibility and enrollment .................................................................................................................................. 144
When medical coverage begins .......................................................................................................................................... 144
Making changes ......................................................................................................................................................................... 146
When medical coverage ends .............................................................................................................................................. 151
General provisions for eligibility and enrollment ....................................................................................................... 154
Eligibility and enrollment for a retiree or survivor .......................................................................................................... 155
Eligibility for subscribers and dependents ..................................................................................................................... 155
Enrollment for subscribers and dependents ................................................................................................................. 157
Medicare eligibility and enrollment .................................................................................................................................. 159
When medical coverage begins .......................................................................................................................................... 160
Making changes ......................................................................................................................................................................... 161
When medical coverage ends .............................................................................................................................................. 166
General provisions for eligibility and enrollment ....................................................................................................... 168
Definitions ......................................................................................................................................................................................... 169
Disclosures ......................................................................................................................................................................................... 192
2024 UMP CDHP (PEBB) Certificate of Coverage 13
Online services
See the Directory pages at the beginning of this booklet for links and contact information.
Visit the UMP website to register for a Regence account and get personalized information such as:
• Access the certificate of coverage (this booklet) and the summary of benefits and coverage (SBC) for
your plan, as well as the Glossary of Health Coverage and Medical Terms.
• Access your online pharmacy account to view prescription claims.
• Chat now with customer service.
• Download the Regence mobile application.
• Find providers in your plan’s network.
• View or order your UMP member ID card.
• View your Explanations of Benefits (EOBs).
• View letters UMP sent you.
Visit the UMP website to:
• Access information on BlueCard® or Blue Cross Blue Shield Global® Core.
• Access resources and programs.
• Access the certificates of coverage (this booklet) and the summaries of benefits and coverage (SBCs)
for all plans.
• Access UMP medical policies.
• Access wellness tools.
• Download or print documents and forms.
• Find providers in any plan network.
• Get cost estimates for treatment of common medical conditions.
• Learn about submitting medical claims.
• Review complaints and appeals procedures.
Visit the Policies that affect your care webpage to:
• View Regence medical policies.
Visit the UMP vision benefits webpage to:
• Find a link to the Vision Service Plan (VSP) website.
• Find information on your vision benefit.
Visit the UMP Prescription drug coverage webpage to:
• Find a link to the UMP Preferred Drug List and the Drug Price Check tool.
• Find a link to your online pharmacy account.
• Find information on mail-order and specialty drugs.
• Learn about submitting prescription drug claims.
• Locate network pharmacies or network vaccination pharmacies.
14 2024 UMP CDHP (PEBB) Certificate of Coverage
• Review prescription drug policies and programs.
Visit the HealthEquity website to:
• Sign in to your personal member portal.
• Check your health savings account (HSA) balance.
• View and pay a provider’s claim that has already been processed by UMP.
• Make deposits directly from your bank account using electronic funds transfer.
• Manage your investments (for accounts with more than $1,500).
• Check your transaction history.
• Find forms or submit an online request to get reimbursed for expenses you paid out of pocket.
• View and print monthly account statements and tax forms.
How to use this certificate of coverage
For general topics, check the table of contents.
For an overview of the most common benefits, see the “Summary of benefits” section. The summary also
shows:
• How much you will pay.
• The page numbers where you may learn more about a benefit.
To look up unfamiliar terms, see the “Definitions” section.
About UMP CDHP
Uniform Medical Plan Consumer-directed Health Plan (UMP CDHP) is a self-insured Preferred Provider
Organization (PPO) health plan. UMP is offered through the Washington State Health Care Authority’s
(HCA’s) Public Employees Benefits Board (PEBB) Program. UMP is administered by Regence BlueShield
and Washington State Rx Services (WSRxS) in partnership with HealthEquity, the trustee (manager) of your
health savings account (HSA). All prescription drugs, services, or other benefit changes may require
approval by the PEB Board. Approval takes place when benefits are procured for the next calendar year.
This plan is available only to people eligible for coverage through the PEBB Program. See the “Eligibility
and Enrollment” section for more information.
This plan is designed to keep you and your enrolled dependents healthy and provide benefits in case of
injury or illness. Review this certificate of coverage (COC) carefully so you may get the most from your
health care benefits.
Features of UMP CDHP
UMP CDHP is a health plan that covers the same services as the UMP Classic plan. However, this plan has
a different payment structure and a higher deductible for covered services for a lower premium.
This plan has one combined deductible for medical services and prescription drugs. If you have one or
more dependents enrolled in your plan, you must pay the total combined family deductible before the
plan pays for services, including prescription drugs. Certain covered preventive care services and covered
insulins are not subject to your deductible, which means the plan will pay for some services before you
meet your deductible. See the “Deductible” section under “What you pay for services” for more
information.
2024 UMP CDHP (PEBB) Certificate of Coverage 15
A major feature of this plan is a tax-free Health Savings Account (HSA). You and your employer may
contribute tax-free money into this savings account to pay for IRS-qualified medical expenses (such as the
deductible and coinsurance), including certain services and certain drugs the plan may not cover.
Contributions remain in your HSA until you use them; the balance rolls over from year-to-year.
If you or your dependents are enrolled in UMP CDHP and want to enroll in another health plan, it must be
another high-deductible health plan, but without an HSA.
When enrolled in UMP CDHP, you may not also be enrolled in any of the following plans:
• Medicare Part A or Part B.
• Medicaid (called “Apple Health” in Washington).
• Another comprehensive medical plan, such as a spouse or state-registered domestic partner’s plan.
• A Voluntary Employees’ Beneficiary Association Medical Expense Plan (VEBA MEP) account, unless you
convert it to a limited VEBA MEP.
• TRICARE.
• The Civilian Health and Medical Program of the Department of Veterans Affairs (CHAMPVA).
• A medical flexible spending arrangement (FSA) or health reimbursement arrangement (HRA). This also
applies if your spouse has a medical FSA, even if you are not covering your spouse on UMP CDHP. This
does not apply to a Limited Purpose FSA.
Accumulators
Insurance accumulators may transfer when a subscriber changes their enrollment from one UMP plan to
another UMP plan mid-year during a special open enrollment (SOE).
When a subscriber enrolled in a PEBB Program UMP plan changes their own enrollment to another PEBB
Program UMP plan (meaning the subscriber continues to be the subscriber on the new PEBB Program
UMP Plan) during an SOE, the amounts already accrued toward medical and pharmacy deductibles, out-
of-pocket limits, and benefit limits (see definition of “Limited benefit”) will transfer to the new PEBB
Program UMP plan. These accumulators will also transfer for any member on the subscriber’s account
who changes UMP plans with the subscriber.
When a subscriber enrolled in a SEBB Program UMP plan changes their enrollment to a PEBB Program
UMP plan (meaning the subscriber continues to be the subscriber on the new PEBB Program UMP Plan)
during an SOE, the amounts already accrued toward the medical and pharmacy deductibles and the out-
of-pocket limits for themselves and their enrolled dependents will transfer to the new PEBB Program UMP
plan. These accumulators will also transfer for any member on the subscriber’s account who changes UMP
plans with the subscriber.
If you have questions, contact UMP Customer Service.
Finding a health care provider
As a UMP member, you may see preferred, participating, or out-of-network providers. The amount you
pay for services depends on the network status of the provider. Seeing preferred providers will save you
money.
Visit the UMP provider search to find UMP CDHP providers. You can search for preferred or participating
providers by signing in to your Regence account and selecting Find a Doctor. See the Directory pages at
the beginning of this booklet for links and contact information.
16 2024 UMP CDHP (PEBB) Certificate of Coverage
If you use Find a Doctor by searching as a guest, you will only see preferred providers. You can confirm a
provider’s network status before your visit by using the provider search or contacting UMP Customer
Service.
Preferred providers are in the Preferred Provider Organization (PPO) network that applies to UMP CDHP
members.
ALERT! Some providers are preferred at one practice location but not another (example:
urgent care clinics). Contact UMP Customer Service if you have any questions about the
network status of a provider at a specific location.
• You pay 15 percent of the allowed amount after you meet your deductible. The plan pays 85 percent of
the allowed amount.
• You pay $0 for covered preventive care services, including covered immunizations. The plan pays 100
percent of the allowed amount.
• The provider cannot bill you for charges above the allowed amount.
• When you are signed in to your Regence account the online provider directory labels preferred
providers with a bar icon and “category 1” like this:
• If you see a preferred provider, you will not have to file a claim if the plan is your primary coverage.
• When you receive nonemergency services at a network hospital, network hospital outpatient
department, network critical access hospital, or network ambulatory surgical center in Washington
State, you pay the network rate and cannot be balance billed regardless of the network status of the
provider. For nonemergency services performed at one of these facilities outside of Washington State,
you still pay the network rate, but in some states, an out-of-network provider may be allowed to ask
you to waive some of your balance billing protections.
ALERT! Some services and supplies are not covered by the plan (see the “What the plan does
not cover” section) or have benefit limits. If you receive services or supplies that are not
covered by the plan or you exceed your benefit limit, you will pay for those services or supplies,
even if you see preferred providers. Contact UMP Customer Service to find out if a service or
supply is covered.
Participating providers contract with Regence BlueShield or another BlueCard® network as a
participating provider.
• You pay 40 percent of the allowed amount after you meet your deductible. The plan pays most covered
services at 60 percent of the allowed amount.
• You pay $0 for covered preventive care services, including covered immunizations. The plan pays 100
percent of the allowed amount.
• The provider cannot bill you for charges above the allowed amount.

2024 UMP CDHP (PEBB) Certificate of Coverage 17
• When you are signed in to your Regence account the online provider directory labels participating
providers with a bar icon and “category 2” like this:
• If you see a participating provider, you will not have to file a claim if the plan is your primary coverage.
Out-of-network providers are not contracted with Regence BlueShield or another BlueCard® network.
• You pay 40 percent of the allowed amount after you meet your deductible. The plan pays most covered
services at 60 percent of the allowed amount.
Note: The provider may bill you for charges above the allowed amount, which is known as balance
billing. You pay all charges billed to you above the allowed amount. Any balance billed amounts do not
apply to your out-of-pocket limit.
At an out-of-network facility, when you receive emergency services you pay the network cost-sharing
amount regardless of the network status of the provider or facility, and cannot be balance billed.
• You pay 40 percent of the allowed amount for covered preventive care services, including covered
preventive immunizations. You will pay all charges above the allowed amount (balance billing). The
plan pays 60 percent of the allowed amount.
• You pay $0 for flu shots and COVID-19 vaccines.
• The plan pays 100 percent of the allowed amount for covered preventive childhood immunizations.
• The 40 percent coinsurance you pay to out-of-network providers will not apply to your deductible or
out-of-pocket limit.
• Any amount you pay above the allowed amount does not apply to your deductible or out-of-pocket
limit.
• You may have to pay all charges at the time of service and then fill-out and send a claim form to the
plan for reimbursement.
• The provider may choose not to request preauthorization for services that require it. As a result, the
plan may delay or deny payment.
Note: The plan may send payment for covered out-of-network services to you or the provider.
Sample payments to different provider network status
The table below shows how much you pay for professional services from preferred, participating, and out-
of-network providers when UMP is your primary medical insurance. For these examples, assume you have
met your deductible and have not reached your out-of-pocket limit. See descriptions of these provider
types beginning on page 15. These are examples only and may not reflect your specific situation.
Provider
type
Must provider accept
allowed amount?
Balance
billing
allowed?
Itemized payments
You owe
provider
Preferred
provider
Yes. You pay 15% of the
allowed amount
(coinsurance).
No
Billed charge: $1,000
Allowed amount: $900
Plan pays 85%: -$765
You pay 15%: $135
$135
18 2024 UMP CDHP (PEBB) Certificate of Coverage
Provider
type
Must provider accept
allowed amount?
Balance
billing
allowed?
Itemized payments
You owe
provider
Participating
provider
Yes. You pay 40% of the
allowed amount
(coinsurance).
No
Billed charge: $1,000
Allowed amount: $900
Plan pays 60%: -$540
You pay 40%: $360
$360
Out-of-
network
provider*
No. You pay 40% of the
allowed amount
(coinsurance), plus all
charges above the
allowed amount.
Yes
Billed charge: $1,000
Allowed amount: $900
Plan pays 60%: -$540
You pay 40% plus
$100** over allowed
amount: $460*
$460*
* This amount does not apply to your out-of-pocket limit.
** When you receive nonemergency services at a network hospital, network hospital outpatient
department, network critical access hospital, or network ambulatory surgical center in Washington State,
you pay the network rate and cannot be balance billed regardless of the network status of the provider.
For nonemergency services performed at one of these facilities outside of Washington State, you still pay
the network rate, but in some states, an out-of-network provider may be allowed to ask you to waive
some of your balance billing protections.
How to find a preferred provider
As a UMP member, you have access to Regence BlueShield preferred providers and Blue Cross and Blue
Shield plan providers worldwide through the Blue Cross Blue Shield Global® Core program (see the
“Services received outside the United States” section). This means your health coverage is with you
wherever you are. Your access to care includes many acute care hospitals, urgent care and ambulatory
surgery centers, physicians, and other health care professionals.
To find a preferred provider, choose one of the following:
• Use the UMP provider search.
• Contact UMP Customer Service.
• Sign in to your Regence account, where you have access to more information about providers, as well
as other tools.
• Use the Regence mobile application to find providers in your network.
• Call Blue Cross Blue Shield Global® Core Service Center at 1-800-810-2583 or call collect at 1-804-673-
1177 to find providers outside the U.S. You can also use the online provider search tool on the Blue
Cross Blue Shield Global Core website at bcbsglobalcore.com.
• Visit the Prescription drug coverage webpage to locate network pharmacies.
See the Directory pages at the beginning of this booklet for links and contact information.
2024 UMP CDHP (PEBB) Certificate of Coverage 19
Covered and noncovered provider types
Covered provider types
The plan pays the allowed amount for covered services only when performed by covered provider types
within the scope of their license(s). When a facility charges facility fees, the plan pays the allowed amount
if the services are covered services and are within the scope of the facility’s license. All preferred and
participating providers are covered provider types.
See the list of covered provider types at the UMP website at
ump.regence.com/pebb/benefits/providers/covered-providers.
Noncovered provider types
If you see a provider who is not a covered provider type, such as a Licensed Athletic Trainer, the plan will
not pay for any of the services received, and you will pay for all charges. As with all noncovered services,
any payments you make to a noncovered provider type will not apply to your deductible or out-of-pocket
limit. If you have questions about noncovered providers contact UMP Customer Service.
Primary care providers
A primary care provider (PCP) is a physician, nurse practitioner, or physician assistant who provides,
coordinates, and helps you access a range of health care services, such as covered immunizations. A PCP
may also help coordinate care for you when you need to see specialists.
You are not required to choose a PCP. However, a PCP may help prevent and treat health care conditions
early, promoting your health and well-being. Patients who have a PCP have better health outcomes and a
better care experience. To be designated as a PCP, a provider must be one of the provider types and
practice under one of the specialties listed below.
Provider type:
• Doctor of Osteopathic Medicine (D.O.)
• Medical Doctor (M.D.)
• Naturopathic Physician (N.D.)
• Nurse Practitioner (A.R.N.P.)
• Physician Assistant (P.A.)
Specialties:
• Adult Medicine
• Family Practice
• General Practice
• Geriatrics
• Internal Medicine
• Obstetrics and gynecology (OB/GYN)
• Pediatrics (for members under age 18)
• Preventive Medicine
When you do not have access to a preferred provider:
network waiver
An approved network waiver allows the plan to pay for covered services provided by an out-of-network
provider at the network rate. You may request a network waiver only when you do not have access to a
preferred provider able to provide covered medically necessary services within 30 miles of your residence.
A service or supply prescribed, ordered, recommended, approved, or given by a provider does not
make it a medically necessary covered service or supply.
20 2024 UMP CDHP (PEBB) Certificate of Coverage
When and how to request a network waiver
Before your visit
When services require preauthorization, you may request a network waiver before services are provided.
Visit the UMP Policies that affect your care webpage for the list of services requiring preauthorization (see
Directory for link). Your network waiver request should be included with the preauthorization request. See
the “Information needed to submit a network waiver request” section to learn what to include in your
request.
When the plan approves the network waiver before you receive medical services from an out-of-network
provider:
• You pay your cost-share for medical services the plan has approved through this waiver as though the
provider is preferred.
• You pay $0 for covered preventive services, including covered immunizations. The plan pays 100
percent of the allowed amount.
After your visit
When you receive any service, except those that require preauthorization, you may request a network
waiver after the claims have been processed.
Network waiver requests not approved in advance are considered an appeal and must be submitted
within 180 days of receiving an Explanation of Benefits. See the “Complaint and appeal procedures”
section for information about your appeal rights.
Information needed to submit a network waiver request
You should include all the following information in your request:
• A letter of explanation from you or your provider stating the need to see the out-of-network provider.
• Details of the research conducted by you or your provider to locate a preferred provider (e.g., dates
network status was checked, names and phone numbers of preferred providers that were researched
and may have been contacted before receiving services from the out-of-network provider).
More information needed for preauthorization requests
When submitting a request for preauthorization that includes a network waiver, all the following
additional information should also be included:
• Performing provider’s name, address, phone number, and National Provider Identifier (NPI) or Tax ID
number (TIN)
• Diagnosis codes
• Procedure codes
• Length of treatment requested or required for services
• Estimated charges
See the “Preauthorizing medical services” section for more information about requesting medical services
preauthorization from the plan.
Where to send your network waiver request
UMP Member Appeals
Regence BlueShield
PO Box 1106
2024 UMP CDHP (PEBB) Certificate of Coverage 21
Lewiston, ID 83501-1106
If you have questions about the network waiver process, contact UMP Customer Service.
ALERT! If a network waiver is approved, you must still pay your cost-share for most medical
services. Services provided under an approved network waiver apply to your deductible and
out-of-pocket limit. Network waivers for ongoing services may require periodic review.
How an HSA works
ALERT! If you enroll in a consumer-directed health plan with an HSA, you can also choose to
enroll in a Limited Purpose Flexible Spending Arrangement (FSA). Limited Purpose FSA funds
can be used only for dental and vision expenses, which allows you to save your HSA funds for
medical expenses. A Limited Purpose FSA is different from a Medical FSA. You may not have a
Medical FSA and an HSA in the same year, as you may be subject to tax penalties.
The subscriber is the owner of the HSA. They get the tax advantages associated with an HSA and pay any
taxes or penalties that result if the HSA does not comply with Internal Revenue Service (IRS) rules. The
subscriber may contribute funds to the HSA within certain limits. Money from the HSA may be used to
pay for qualified medical expenses of the subscriber, spouse or tax dependents (claimed as a tax
dependent), even if they are not enrolled in this plan. See page 27 for details of how this works with UMP
CDHP.
The trustee (manager) of your HSA, HealthEquity, features a member portal on their website (see
Directory for link). When you sign into your Regence account, you may also find a link to the HealthEquity
portal. Find out which services are available in the portal by reading the “Online services” section.
ALERT! You and your dependents may only enroll in other high-deductible health plans that
do not include an HSA.
Out-of-area services
Regence BlueShield has a variety of relationships with other Blue Cross and/or Blue Shield Licensees.
Generally, these relationships are called “Inter-Plan Arrangements.” These Inter-Plan Arrangements work
based on rules and procedures issued by the Blue Cross Blue Shield Association. Whenever you access
health care services outside of the geographic area Regence BlueShield services, the claim for those
services may be processed through one of these Inter-Plan Arrangements. The Inter-Plan Arrangements
are described below.
When you receive care outside of Regence BlueShield’s service Area, you may receive it from Providers as
described below. Providers contracted with the local Blue Cross and/or Blue Shield Licensee in that
geographic area ("Host Blue") as a preferred provider are paid at the preferred provider level and will not
bill you for balances beyond any deductible, copayment and/or coinsurance for covered services.
Providers that contract with the Host Blue as a participating provider are paid at the participating provider
level and will not bill you for balances beyond any deductible, copayment and/or coinsurance for covered
22 2024 UMP CDHP (PEBB) Certificate of Coverage
services. Some providers (out of network providers) don't contract with the Host Blue. The section below
explains how the Plan pays these different kinds of providers.
BlueCard® Program
Under the BlueCard® Program, when you access covered services within the geographic area served by a
Host Blue, Regence will remain responsible for doing what was agreed to in the contract. However, the
Host Blue is responsible for contracting with and generally handling all interactions with its preferred or
participating providers.
When covered services are received outside the Regence’s service area and the claim is processed
through the BlueCard® Program, the amount you pay for covered services is calculated based on the
lower of:
• The billed covered charges for your covered services; or
• The negotiated price that the Host Blue makes available to Regence.
Often, this “negotiated price” will be a simple discount that reflects an actual price that the Host Blue pays
to your health care provider. Sometimes, it is an estimated price that considers special arrangements with
your health care provider or provider group that may include types of settlements, incentive payments,
and/or other credits or charges. Occasionally, it may be an average price, based on a discount that results
in expected average savings for similar types of health care providers after considering the same types of
transactions as with an estimated price.
Estimated pricing and average pricing, going forward, also take into account adjustments to correct for
over- or underestimation of modifications of past pricing of claims, as noted above. However, such
adjustments will not affect the price Regence BlueShield uses for your claim because they will not be
applied after a claim has already been paid.
Laws in a small number of states may require the Host Blue to add a surcharge to your calculation. If any
state laws mandate other liability calculation methods, including a surcharge, Regence would then
calculate your liability for any covered services according to applicable law.
Value Based Programs
If covered services are received under a Value-Based Program inside a Host Blue's service area, you will
not be responsible for paying any of the provider incentives, risk-sharing, and/or care coordinator fees
that are a part of such an arrangement, except when a Host Blue passes these fees to the Regence
through average pricing or fee schedule adjustments.
For the purpose of this section, the following definitions apply.
Value-Based Program: An outcomes-based payment arrangement and/or a coordinated care model
facilitated with one or more local providers that is evaluated against cost and quality metrics/factors and
is reflected in provider payment.
Provider Incentive: An additional amount of compensation paid to a healthcare provider by a Blue Cross
and/or Blue Shield Plan, based on the provider's compliance with agreed-upon procedural and/or
outcome measures for a particular group of covered persons.
A Care Coordination Fee is a fixed amount paid by a Blue Cross and/or Blue Shield Licensee to Providers
periodically for Care Coordination under a Value-Based Program.
2024 UMP CDHP (PEBB) Certificate of Coverage 23
Inter-Plan Programs: Federal or state taxes, surcharges, or
fees
Federal law or state law may require a surcharge, tax or other fee that applies to self-insured accounts. If
applicable, any such surcharge, tax or other fee will be included as part of the claim fee passed on to the
claimant.
Out-of-network providers outside Regence’s service area
Member liability
When covered services are provided outside of Regence’s service area by out-of-network providers, the
amount you pay for such services will generally be based on either the Host Blue’s out-of-network
provider local payment or the pricing arrangements required by applicable state law. In these situations,
you may be liable for the difference between the amount that the out-of-network provider bills and the
payment Regence will make for the covered services as set forth in this paragraph. Federal or state law, as
applicable, will govern payments for nonparticipating emergency services.
Exceptions
In certain situations, Regence may use other payment bases such as billed covered charges, the payment
Regence would make if the health care services had been obtained within Regence’s service area, or a
special negotiated payment, as permitted under Inter-Plan Programs Policies, to determine the amount
Regence will pay for services rendered by out-of-network providers. In these situations, you may be liable
for the difference between the amount that the out-of-network provider bills and the payment Regence
will make for the covered services as set forth in this paragraph.
Services received outside the United States
ALERT! The plan does not cover prescription drugs ordered through mail-order pharmacies
located outside the U.S. See “Prescription drugs purchased outside the U.S.” on page 96 to
learn more.
Blue Cross Blue Shield Global® Core
ALERT! Claims for services received outside the U.S. may take longer to process. UMP
Customer Service is available to assist members with the Global® Core claim process.
If you are outside the U.S., you may be able to take advantage of Blue Cross Blue Shield Global® Core
when accessing covered health services. Blue Cross Blue Shield Global® Core is unlike the BlueCard®
Program available in the U.S. in certain ways. For instance, although the Blue Cross Blue Shield Global®
Core assists you with accessing a network of inpatient, outpatient, and professional providers, the network
is not served by a Host Blue. As such, when you receive care from providers outside the U.S., you will
typically have to pay the providers and submit the claims yourself to obtain reimbursement for these
services.
If you need medical services (including locating a doctor or hospital) outside the U.S., you should call the
service center at 1-800-810-BLUE (2583) or call collect at 1-804-673-1177, 24 hours a day, 7 days a week.
An assistance coordinator, working with a medical professional, will arrange a physician appointment or
hospitalization, if necessary.
24 2024 UMP CDHP (PEBB) Certificate of Coverage
Inpatient services
In most cases, if you contact the service center for assistance, hospitals will not require you to pay upfront
for covered inpatient services, except for your medical deductible, coinsurance, and copays. In such cases,
the hospital will submit your claims to the service center to begin claims processing. However, if you paid
in full at the time of services, you must submit a claim to receive reimbursement for covered health care
services.
Outpatient services
Physicians, urgent care centers, and other outpatient providers located outside the U.S. will typically
require you to pay in full at the time of services. You must submit a claim to obtain reimbursement for
covered health care services.
Submitting a Blue Cross Blue Shield Global® Core claim
When you pay for covered health care services outside the BlueCard® service area, you must submit a
claim to obtain reimbursement. For institutional and professional claims, complete a Blue Cross Blue
Shield Global® Core claim form and send the claim form with the provider's itemized bill(s) to the service
center (the address is on the form) to initiate claims processing. Following the instructions on the claim
form will help ensure timely processing of your claim. The claim form is available from the claims
administrator, the service center, or online at the Blue Cross Blue Shield Global Core® website at
bcbsglobalcore.com. If you need assistance with your claim submission, you should call the service center
at 1-800-810-BLUE (2583) or call collect at 1-804-673-1177, 24 hours a day, 7 days a week.
When services received outside the U.S. are covered
The plan covers the same benefits as described in this COC if the services received outside the U.S.:
• Are appropriate for the condition being treated;
• Are covered by the plan;
• Are medically necessary;
• Are not considered to be experimental or investigational by U.S. standards; and
• Have met all medical policy criteria.
Important tips for receiving care outside the U.S.
• Always carry your UMP member ID card.
• If you need emergency medical care, go to the nearest hospital.
• If you need urgent medical care, contact the Blue Cross Blue Shield Global® Core Service Center for
help finding a network provider.
• If you are admitted to the hospital, contact the Blue Cross Blue Shield Global® Core Service Center to
notify the plan of your admission.
Blue Cross Blue Shield Global® Core contact and online
information
Contact Blue Cross Blue Shield Global® Core to learn about services received outside the U.S., find a
provider outside the U.S., or submit a claim for medical care provided outside the U.S.
• Call the Blue Cross Blue Shield Global® Core Service Center at 1-800-810-BLUE (2583), or call collect
1-804-673-1177 (available 24 hours a day, 7 days a week).
• To use the online provider search tool, register and sign in on the Blue Cross Blue Shield Global® Core
website at bcbsglobalcore.com.

2024 UMP CDHP (PEBB) Certificate of Coverage 25
• Visit the Blue Cross Blue Shield Global® Core website on the Blue Cross Blue Shield Global® Core
website at bcbsglobalcore.com. After you create an account, you may find Blue Cross Blue Shield
Global® Core information, get an international claim form, and submit claims electronically.
Finding a preferred provider outside the U.S.
Under Blue Cross Blue Shield Global® Core, you have access to network providers outside the U.S.,
including hospital care (inpatient and outpatient) and professional provider services at network rates.
To find a contracted provider outside the U.S., register and sign in on the Blue Cross Blue Shield Global®
Core website at bcbsglobalcore.com or call the Blue Cross Blue Shield Global® Core Service Center:
1-800-810-BLUE (2583) or collect at 1-804-673-1177.
What you pay for services
Deductible
A deductible is a fixed dollar amount you pay each calendar year before the plan begins paying for
covered services. The deductible is combined for medical services and prescription drugs.
Your deductible amount depends on the number of people enrolled in your plan:
• For subscriber only (one member) it is $1,600;
• For subscriber plus one or more dependents (two or more members), it is $3,200.
Your deductible applies to all services, including prescription drugs paid by the member directly or paid
on behalf of the member by another person including payments made through a manufacturer drug
coupon or other manufacturer discount, unless otherwise stated in this COC. See below for services that
are not subject to your deductible. Services apply to your UMP deductible in the order claims are received,
not necessarily in the order the member receives the services.
ALERT! If you receive services with a benefit limit (such as nutritional counseling) before
meeting your deductible, those visits still apply to the benefit limit. For example, if you pay out
of pocket for a nutritional counseling visit because you have not met your deductible, that visit
will apply to the maximum of 12 visits per lifetime. See definition of “Limited benefit” for more
information.
What does not count toward your deductible
The following out-of-pocket expenses do not count toward your deductible:
• Charges for services that exceed the benefit limit.
• Charges that exceed the maximum dollar limit.
• Out-of-network provider charges above the allowed amount (see the “Sample payments to different
provider network status” section).
• Out-of-pocket costs for services that are not subject to your deductible, except when you pay for
covered insulins. For example, covered preventive care received from an out-of-network provider.
• Services you pay for that are not covered by the plan (see the “What the plan does not cover” section).

26 2024 UMP CDHP (PEBB) Certificate of Coverage
TIP: You may use money from your HSA to pay for noncovered services if they are qualified
medical expenses.
Services not subject to your deductible
The plan pays the allowed amount for the services listed below, subject to cost-share, even if you have not
met your deductible. When you see a preferred or participating provider, you do not have to meet your
deductible before the plan pays for these services:
• Blood pressure monitor if you have a diagnosis of high blood pressure.
• Certain medications covered through the prescription drug benefit as outlined on the UMP Preferred
Drug List.
• Continuous glucose monitors.
• Covered contraceptive supplies and services for women.
• Covered preventive care, including covered immunizations.
• Diabetes Control Program.
• Diabetes Prevention Program.
• Glucometers.
• Hemoglobin A1c testing, and retinopathy screening if you have a diagnosis of diabetes.
• International Normalized Ratio (INR) testing if you have a diagnosis of liver disease and/or bleeding
disorders.
• Low-Density Lipoprotein (LDL) testing if you have a diagnosis of heart disease.
• Peak flow meter if you have a diagnosis of asthma.
• Second opinions required by the plan.
• Tobacco cessation services.
How your deductible works
If you cover yourself only, your deductible is $1,600. You must pay this amount for covered services
subject to the deductible (including covered prescription drugs) before the plan begins to pay for covered
services.
If you cover yourself and at least one other dependent, your deductible is $3,200. You and your
dependent(s) combined must pay this amount for covered services subject to the deductible (including
covered prescription drugs) before the plan begins to pay for covered services. You must pay this amount
for covered services for all covered persons combined before the plan pays for any services, including
prescription drugs (other than those not subject to the deductible). Once the deductible is met, the plan
begins paying for covered services.
Note: Only services that are covered and subject to the deductible count toward the deductible. See the
“What does not count toward the deductible” page 25 for a list of services that do not count toward the
deductible.

2024 UMP CDHP (PEBB) Certificate of Coverage 27
Coinsurance
TIP: Allowed amount is the most the plan pays for a specific covered service or supply. Out-of-
network providers may charge more than this amount, and you are responsible for paying the
difference between the billed amount and the allowed amount. This is called balance billing.
Coinsurance is the percentage of the allowed amount you pay for most medical services and for
prescription drugs when the plan pays less than 100 percent. After you meet your deductible, you pay the
percentages described below for most covered medical services. See the “What you pay for prescription
drugs” section for how much you pay for prescription drugs.
• For preferred providers: You pay 15 percent of the allowed amount. The plan pays 85 percent of the
allowed amount.
• For participating providers: You pay 40 percent of the allowed amount. The plan pays most covered
services at 60 percent of the allowed amount.
• For out-of-network providers: You pay 40 percent of the allowed amount, and the provider may
balance bill you. The plan pays most covered services at 60 percent of the allowed amount.
Professional charges, such as for physician services while you are in the hospital or lab work, may be billed
separately.
Note: When you receive nonemergency services at a network hospital, network hospital outpatient
department, network critical access hospital, or network ambulatory surgical center in Washington State,
you pay the network rate and cannot be balance billed regardless of the network status of the provider.
For nonemergency services performed at one of these facilities outside of Washington State, you still pay
the network rate, but in some states, an out-of-network provider may be allowed to ask you to waive
some of your balance billing protections.
At an out-of-network facility, when you receive emergency services you pay the network cost-sharing
amount regardless of the network status of the provider or facility and cannot be balance billed.
When you pay
Most of the time, you pay after your claim is processed.
• You will receive an Explanation of Benefits (EOB) from the plan that explains how much the plan paid
the provider. The Member Responsibility section of your EOB tells you how much you owe the provider.
• The provider sends you a bill.
• You pay the provider.
Note: A provider may ask you to pay your deductible, when applicable, at the time of service. When this
happens, check your EOB to make sure the amount you paid is accurately reflected in the Member
Responsibility section. Contact UMP Customer Service with questions.
Health savings account (HSA)
The State of Washington will contribute $700.08 for one person, and $1,400.04 for more than one person
enrolled in the plan, deposited in equal amounts over the calendar year. Employer contributions are made
only during those months you are enrolled in UMP CDHP. You may also make contributions to your HSA
account. To confirm the maximum annual contribution limits, visit the IRS website at irs.gov/government-
entities/federal-state-local-governments/where-can-i-learn-more-about-health-savings-accounts-hsa-
28 2024 UMP CDHP (PEBB) Certificate of Coverage
and-health-reimbursement-arrangements-hra. The State of Washington’s contributions apply to the
limits, as does the SmartHealth wellness incentive (see page 28).
You may use your HSA to pay for member cost-sharing and other qualified medical expenses as described
in Internal Revenue Code (IRC) 223(d)(2), including expenses not normally covered by the plan. You may
use HSA funds to pay for expenses for your spouse or tax dependents, even if they are not covered by the
plan. The IRS determines which services are eligible for reimbursement through an HSA, and who may pay
for services using HSA funds. For details on how to use your HSA, including a list of items and services
that you may pay for with your HSA funds, visit the HealthEquity website or contact HealthEquity (see
Directory for link and contact information).
If you earned the SmartHealth wellness incentive
Eligible subscribers can qualify for a one-time $125 into their HSA (if enrolled in a consumer-directed
health plan in 2024). If you qualified in 2023 and you are still eligible to participate in the wellness
incentive program, the incentive is distributed in January 2024. More details on eligibility and program
requirements are on HCA's SmartHealth webpage at hca.wa.gov/pebb-smarthealth.
How to pay using your HSA
After a claim is processed, you may sign in to your HealthEquity HSA to view your medical claims.
However, you will not be able to view your pharmacy claims.
You may pay for qualified medical expenses (see the definition of “Qualified medical expense”) and
qualified prescription drug expenses by:
• Using your HealthEquity debit card at the time of service.
• Logging in to your HSA and designating payment to be sent by HealthEquity directly to the provider.
However, this option is not available for pharmacy claims. Note: You may make a partial payment using
this method.
• Logging in to your HSA and paying yourself back for a qualified medical expense and a qualified
prescription drug expense you paid using non-HSA funds. For example, if you paid cash at your
provider’s office for qualified medical expenses, you may reimburse yourself from your HSA. Reminder:
Pharmacy claims will not be displayed.
Out-of-pocket limit
The out-of-pocket limit is the most you pay during a calendar year for covered services from preferred
providers. The out-of-pocket limit is combined for medical and prescription drugs. After you meet your
out-of-pocket limit for the year, the plan pays for covered services by preferred providers at 100 percent
of the allowed amount. The plan will not pay more than the allowed amount. Expenses are counted from
January 1, 2024, or your first day of enrollment (whichever is later) through December 31, 2024, or
your last day of enrollment (whichever is earlier).
Your out-of-pocket limit depends on the number of persons enrolled in the plan:
• Subscriber only (one member) enrolled: $4,200
• Subscriber plus one or more dependents (two or more members enrolled): $8,400. Once a member
meets $7,000 in covered out-of-pocket expenses annually, the plan will pay for covered services at 100
percent for that member.
What counts toward this limit
• Coinsurance for covered prescription drugs paid by the member directly or paid on behalf of the
member by another person including payments made through a manufacturer drug coupon or other
manufacturer discount.

2024 UMP CDHP (PEBB) Certificate of Coverage 29
• Your coinsurance paid to preferred and participating providers
• Your coinsurance paid to out-of-network providers for emergency room services, air ambulance, and
nonemergency services furnished during a visit or stay at a preferred and participating hospital,
hospital outpatient department, critical access hospital, or ambulatory surgical center.
• Your deductible paid to preferred and participating providers
• Your copay for chiropractic, acupuncture, and massage therapy visits after you meet your deductible
What does not count toward this limit
A. Amounts paid by the plan, including services covered in full
B. Your monthly premiums
C. Your coinsurance paid to out-of-network providers (except those listed above in “What counts toward
this limit”)
D. Balance billed amounts
E. Amounts paid for services the plan does not cover (see the “What the plan does not cover” section)
F. Amounts that are more than the maximum dollar amount paid by the plan. Any amount you pay over
the allowed amount does not count toward the out-of-pocket limit.
G. Amounts paid for services over a benefit limit. For example, the benefit limit for acupuncture is 24
visits. If you have more than 24 acupuncture visits in one year, you will pay in full for those visits, and
what you pay will not count toward this limit.
What you pay after reaching this limit
After you meet your out-of-pocket limit for the year, you pay:
• $0 of the allowed amount for covered medical services from preferred providers and for covered drugs
at network pharmacies.
• B through G (above) in the “What does not count toward this limit” section.
• 40% of the allowed amount for covered medical services for participating providers.
• 40% of the allowed amount for covered medical services for out-of-network providers. You may be
balance billed.
Summary of services and payments
ALERT! Even if a provider orders a test or prescribes a treatment, the plan may not cover it.
Review this COC or contact UMP Customer Service if you have questions about benefits or
limitations.
On the next several pages, you will find a summary of types of services and what you will pay for them.
For a complete understanding of how a benefit works, read the pages listed in the “For more information”
column.
All services must be medically necessary to be covered. If you see an unfamiliar term, see the
alphabetical list of definitions in the “Definitions” section.

30 2024 UMP CDHP (PEBB) Certificate of Coverage
This COC applies only to dates of service between the day your coverage begins (no earlier than January
1, 2024) and the day your coverage ends (no later than December 31, 2024).
ALERT! If you have coverage under another health plan, see the “If you have other HDHP
coverage” section.
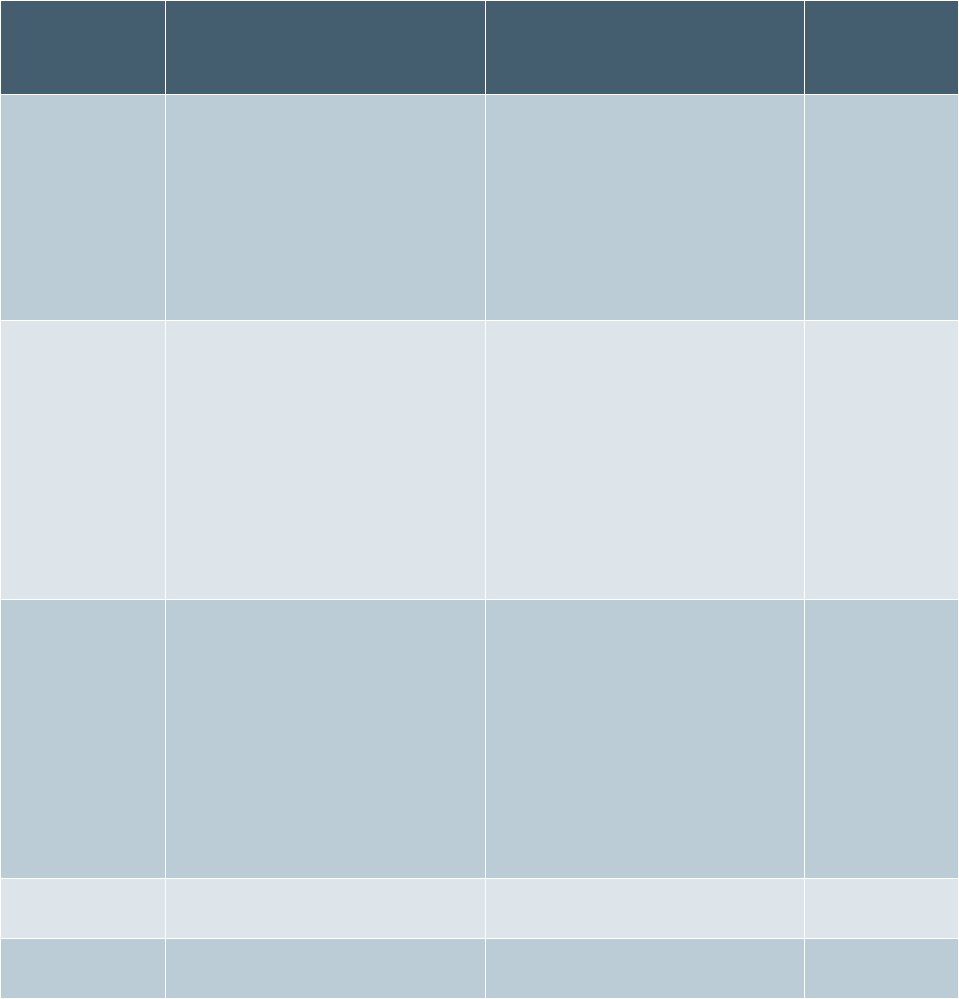
2024 UMP CDHP (PEBB) Certificate of Coverage 31
Deductible and limits
Deductible
and limits
Dollar amounts
What else you need to know
For more
information,
see page(s)
Deductible
$1,600 per member (maximum of
$3,200 for a family of two or
more) Combined deductible for
medical services and prescription
drugs.
See page 28 if you earned the
SmartHealth wellness incentive in
2023 for plan year 2024.
You must meet your deductible
before the plan pays for covered
medical services and covered
prescription drugs. Not all
services count toward this
deductible. There is no
deductible for covered insulins.
25–27
Out-of-pocket
limit
$4,200 per member (maximum of
$8,400 for a family of two or
more) Combined out-of-pocket
limit for medical services and
prescription drugs.
Once a member meets $7,000 in
covered out-of-pocket expenses
annually, the plan will pay for
covered services at 100 percent
for that member.
Your deductible and all
coinsurance for all covered
medical services and covered
prescription drugs paid to
preferred providers count toward
this limit. Once you meet your
out-of-pocket limit, covered
services paid to preferred
providers are paid at 100% of the
allowed amount.
28–29
Health savings
account (HSA)
To confirm the maximum annual
contribution, visit the
IRS website at
irs.gov/government-
entities/federal-state-local-
governments/where-can-i-learn-
more-about-health-savings-
accounts-hsa-and-health-
reimbursement-arrangements-
hra
You may pay for any qualified
medical expenses from your HSA,
including:
• Services that apply to your
deductible.
• Services that are not covered
by the plan but are still
qualified medical expenses.
27
Annual plan
payment limit
None
No limit to how much the plan
pays per calendar year.
Not applicable
Lifetime plan
payment limit
None
No limit to how much the plan
pays over a lifetime.
Not applicable
Types of services
The table in this section describes how much you and the plan will pay for covered services. Unless
otherwise noted, all payments are based on the allowed amount, and services are subject to the
deductible. Unless stated otherwise, services received are subject to your deductible. See the “Deductible”
section for more information about deductibles.
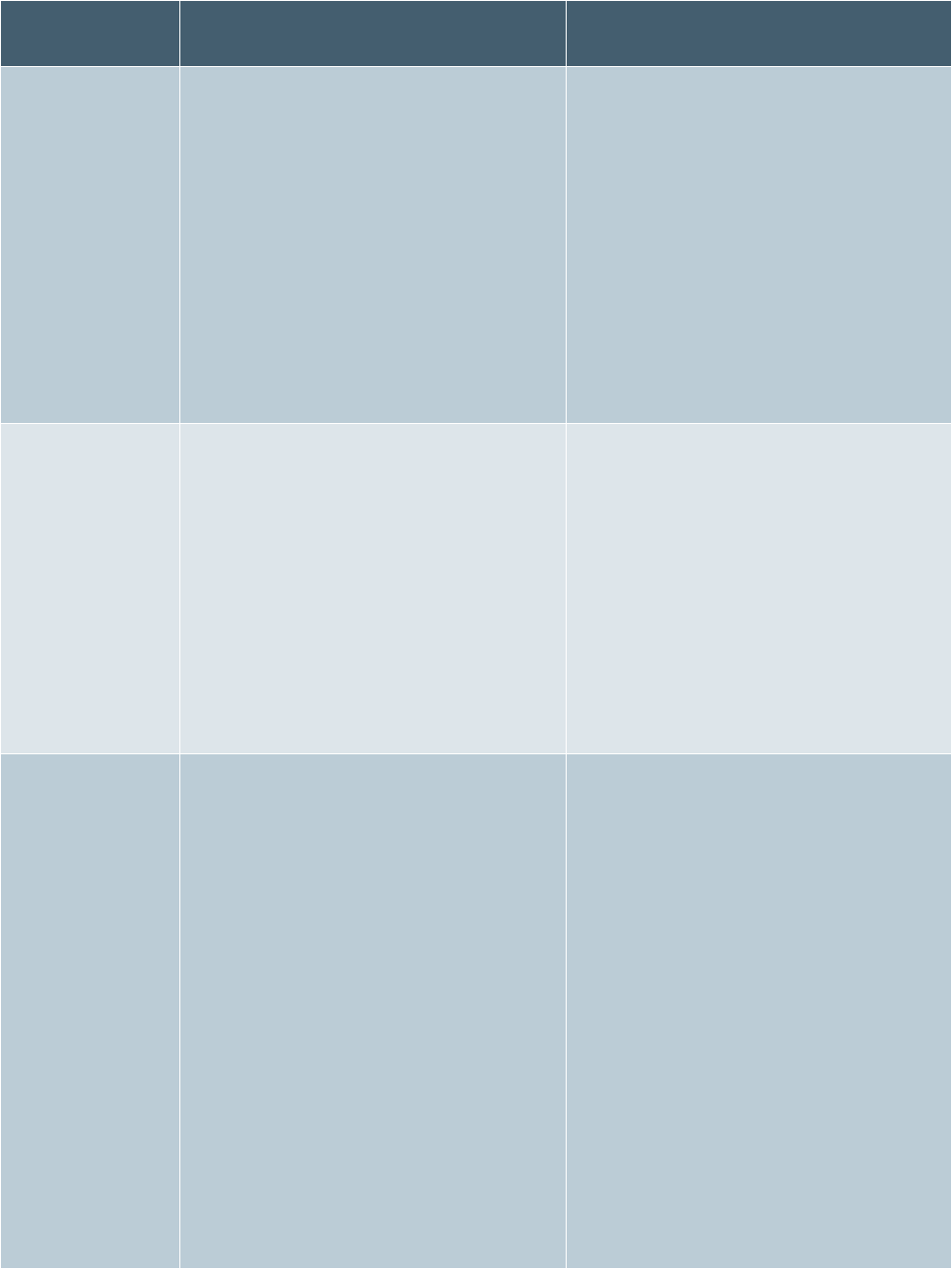
32 2024 UMP CDHP (PEBB) Certificate of Coverage
Type of service
How much you pay for covered
services
How much the plan pays for covered
services
Standard
How much you pay (your coinsurance)
depends on the provider’s network
status:
• Preferred providers: You pay 15% of
the allowed amount. The provider
cannot balance bill you.
• Participating providers: You pay 40%
of the allowed amount. The provider
cannot balance bill you.
• Out-of-network providers: You pay
40% of the allowed amount. The
provider may balance bill you.
• Preferred providers: The plan pays
85% of the allowed amount.
• Participating providers: The plan
pays 60% of the allowed amount.
• Out-of-network providers: The plan
pays 60% of the allowed amount.
Preventive
Covered preventive services are not
subject to your deductible. How much
you pay (your coinsurance) depends on
the provider’s network status:
• Preferred providers: You pay $0. The
provider cannot balance bill you.
• Participating providers: You pay $0.
The provider cannot balance bill you.
• Out-of-network providers: You pay
40% of the allowed amount. The
provider may balance bill you.
• Preferred providers: The plan pays
100% of the allowed amount.
• Participating providers: The plan
pays 100% of the allowed amount.
• Out-of-network providers: The plan
pays 60% of the allowed amount.
Inpatient
Most inpatient services require both
preauthorization (see page 103) and
notice (your provider must notify the plan
as soon as possible after you are
admitted to a facility, but not later than
24 hours after you are admitted; see page
104).
Services are considered inpatient only
when you are admitted to a facility. See
definition of “Inpatient stay” on page 178.
When you are admitted to a facility, you
pay your deductible and:
• Preferred facilities: You pay 15% of
the allowed amount. The provider
cannot balance bill you.
• Participating facilities: You pay 40%
of the allowed amount. The provider
cannot balance bill you.
The plan pays 100% of the allowed
amount after you pay your deductible at
preferred facilities.
The plan pays for professional services
such as provider consultations or lab
tests, based on the provider’s network
status:
• Preferred providers: The plan pays
85% of the allowed amount.
• Participating providers: The plan
pays 60% of the allowed amount.
• Out-of-network providers: The plan
pays 60% of the allowed amount.
2024 UMP CDHP (PEBB) Certificate of Coverage 33
Type of service
How much you pay for covered
services
How much the plan pays for covered
services
• Out-of-network facilities: You pay
40% of the allowed amount. The
provider may balance bill you.
• Fees for professional services, such as,
but not limited to, provider
consultations or lab tests.
How much you pay for professional
services depends on the provider’s
network status:
• Preferred providers: You pay 15% of
the allowed amount. The provider
cannot balance bill you.
• Participating providers: You pay 40%
of the allowed amount. The provider
cannot balance bill you.
• Out-of-network providers: You pay
40% of the allowed amount. The
provider may balance bill you.
Outpatient
If you receive services at a facility that
offers inpatient services (like a hospital)
but you are not admitted, the services are
covered as outpatient. See the specific
benefit (e.g., emergency room or
diagnostic tests) for how much you pay.
You may be billed separately for facility
fees in addition to provider fees.
• Preferred providers: You pay 15% of
the allowed amount. The provider
cannot balance bill you.
• Participating providers: You pay 40%
of the allowed amount. The provider
cannot balance bill you.
• Out-of-network providers: You pay
40% of the allowed amount. The
provider may balance bill you.
• Preferred providers: The plan pays
85% of the allowed amount.
• Participating providers: The plan
pays 60% of the allowed amount.
• Out-of-network providers: The plan
pays 60% of the allowed amount.
34 2024 UMP CDHP (PEBB) Certificate of Coverage
Type of service
How much you pay for covered
services
How much the plan pays for covered
services
Facility
You may be charged facility fees in
addition to provider fees when accessing
clinics, ambulatory surgery centers, and
other facilities. A facility may be referred
to as a “provider” on the Explanations of
Benefits or other documents. How much
you pay depends on the provider’s
network status:
• Preferred facility: You pay 15% of the
allowed amount; the provider cannot
balance bill you.
• Participating facility: You pay 40% of
the allowed amount; the provider
cannot balance bill you.
• Out-of-network facility: You pay 40%
of the allowed amount; the provider
may balance bill you.
• Preferred facility: The plan pays 85%
of the allowed amount.
• Participating facility: The plan pays
60% of the allowed amount.
• Out-of-network facility: The plan
pays 60% of the allowed amount.
Special
These services have unique payment
rules, which are described in the “How
much you will pay” column in the
Summary of benefits table located in the
“Summary of benefits” section.
What else you need to know
• Some services are not covered (see the “What the plan does not cover” section).
• There is no waiting period for preexisting conditions.
• You will save money by seeing preferred providers (see the “Finding a health care provider” section).
• You must be enrolled in this plan for the plan to pay for medically necessary covered services.
Benefits: what the plan covers
Guidelines for coverage
ALERT! A service or supply prescribed, ordered, recommended, approved, or given by a
provider does not make it a medically necessary covered service or supply.
This plan will cover a service or supply, if it meets all of the following conditions. The service or supply
must:
• Be listed as covered; and
• Be medically necessary; and

2024 UMP CDHP (PEBB) Certificate of Coverage 35
• Be received by a member on a day between the date coverage begins (but no sooner than January 1,
2024) and the date coverage ends (but no later than December 31, 2024); and
• Have been determined to be a covered benefit by the Health Technology Clinical Committee (HTCC), if
reviewed by the HTCC, and, if determined to be covered with conditions, meet the conditions of
coverage established by the HTCC; and
• Meet the plan’s coverage policies and preauthorization requirements.
Limits and exclusions may apply to plan benefits. See both the benefit description and the “What the plan
does not cover” section.
Some services require preauthorization and/or notice before you receive treatment. Visit the UMP Policies
that affect your care webpage for a list of these services, or contact UMP Customer Service to ask if a
certain service is covered, requires preauthorization, or requires notice. See Directory for link and contact
information.
The following sections describe the benefits provided by this plan. Be sure to read them carefully for
important information that may help you get the most from your health coverage. If you do not
understand the benefits, it is your responsibility to ask for help before receiving services by contacting
UMP Customer Service.
UMP CDHP is a self-insured PPO health plan. UMP is offered through HCA’s Public Employees Benefits
Board (PEBB) Program. UMP is administered by Regence BlueShield, and Washington State Rx Services
(WSRxS). All prescription drugs, services, or other benefit changes may require approval by the PEB Board.
Approval takes place when benefits are procured for the next calendar year. For example, prescription
drugs newly approved by the U.S. Food and Drug Administration (FDA) may require approval by the PEB
Board before the plan will cover them.
Health Technology Clinical Committee (HTCC)
ALERT! HTCC determinations may be implemented by the plan at any time during the calendar
year, but are often implemented the January following the HTCC’s decision. HTCC decisions are
posted on the HCA website at hca.wa.gov/hta. Contact UMP Customer Service if you have
questions about specific services that the HTCC has reviewed.
Created by chapter 70.14 of the Revised Code of Washington (RCW), the HTCC is a committee of 11
independent health care professionals that reviews selected health technologies (services) to determine
appropriate coverage, if any, for the services. These may include medical or surgical devices and
procedures, medical equipment, and diagnostic tests.
In public meetings, the HTCC considers public comments and scientific evidence regarding the safety,
medical effectiveness, and cost-effectiveness of the services when making its determination.
How HTCC decisions affect UMP benefits
Under state law, the plan must comply with HTCC decisions, RCW 70.14.120 (1)(a), unless such
determination conflicts with federal or state law. Services reviewed by the HTCC are either covered,
covered with conditions, or not covered. The HTCC determines the conditions, if any, under which the
service will be included as a covered benefit and, if covered, the criteria the plan must use to decide
whether the service is medically necessary. Criteria established by the HTCC take precedence over
Regence’s medical policies. When the HTCC determines that a service is not covered, then the service is
not covered by the plan. Some HTCC decisions include a requirement to follow FDA or Centers for
36 2024 UMP CDHP (PEBB) Certificate of Coverage
Medicare and Medicaid Services (CMS) guidelines. You may review these guidelines on the FDA website at
fda.gov or CMS website at cms.gov.
Where to find HTCC decisions
You may view the list of services that the HTCC has reviewed or currently has under review on the HCA
website at hca.wa.gov/hta. The website includes:
• Evidence reports
• Instructions on providing public comments on pending reviews or re-reviews
• Public comments
• The decisions and criteria for coverage
• The public meeting schedule
You may also contact UMP Customer Service with questions about coverage of conditions for HTCC
technologies.
Summary of benefits
ALERT! Not all covered services and limitations are listed in the table below. See the
alphabetical list of all covered services in the “List of benefits” section and see the “Your routine
vision benefit” section.
Read the pages listed in the “For information” column for detailed information about each benefit. Not all
details are included in the table. Also read:
• Services for which your provider must notify the plan (see page 104)
• Services that are not covered (exclusions) (see the “What the plan does not cover” section)
• Services that require preauthorization (see the “Limits on plan coverage” section)
If you have questions about your benefits, benefit limitations, services that require preauthorization or
notice, or services not covered by the plan, contact UMP Customer Service.
For a description of the types of services listed in the “How much you will pay” column in the table below,
see the “Types of services” section. For definitions of the rates, see the definitions of “Inpatient rate,”
“Preventive rate,” “Special rate,” and “Standard rate.”
Benefit/service
How much you will pay
For information,
see page(s):
Ambulance
Special rate:
• 20% of the allowed amount for any provider
• Applies to your out-of-pocket limit
39, 106, 114
Applied Behavior
Analysis (ABA)
Therapy
Standard rate
40
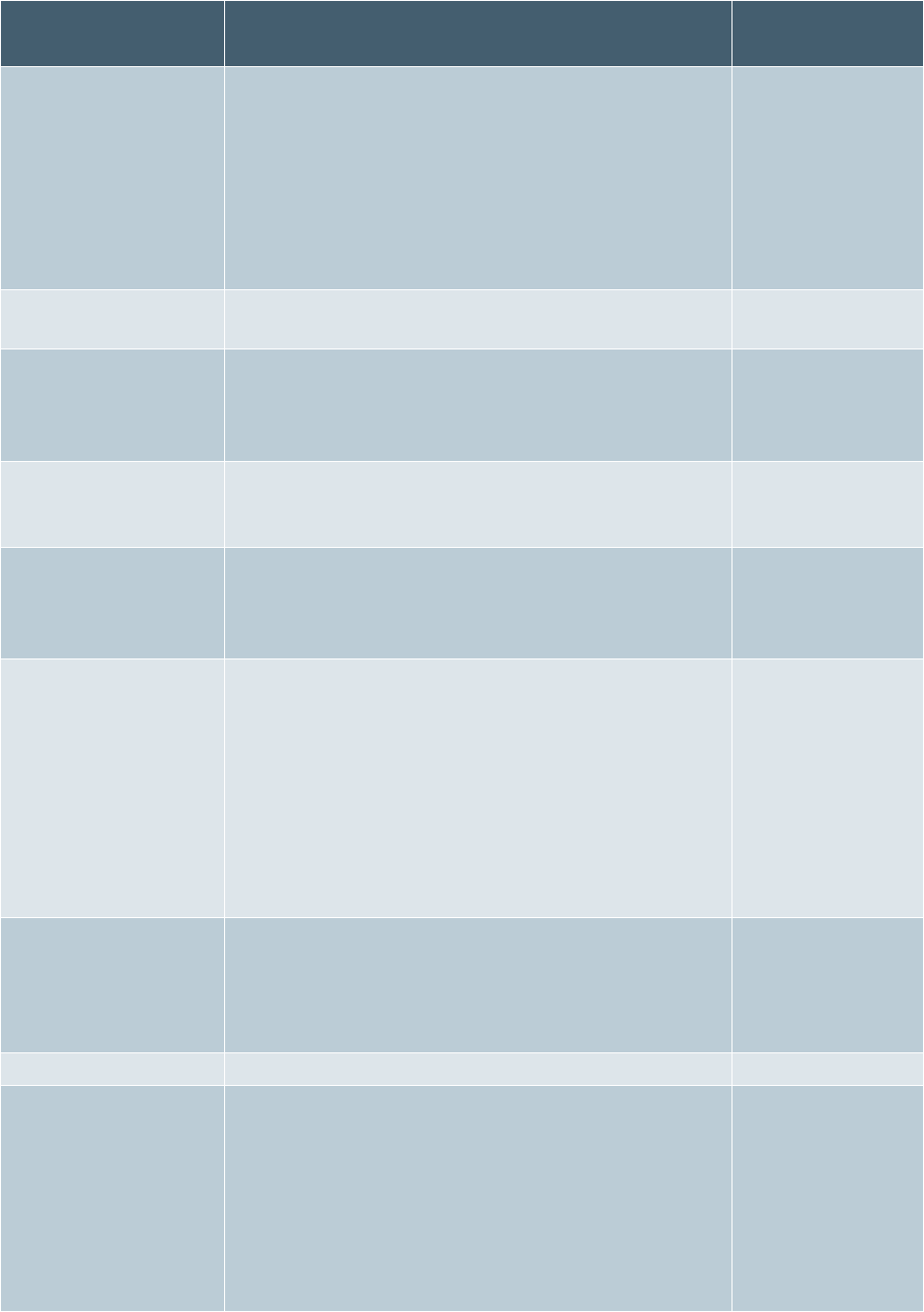
2024 UMP CDHP (PEBB) Certificate of Coverage 37
Benefit/service
How much you will pay
For information,
see page(s):
Behavioral health
Mental health:
• Inpatient rate
• Outpatient/professional services: Standard rate
Substance use disorder:
• Inpatient rate
• Outpatient/professional services: Standard rate
41, 110, 112
Breast health
screening tests
See the “Mammogram and Digital Breast
Tomosynthesis (DBT)” benefit
44, 61
Chiropractic
physician services
See the “Spinal and extremity manipulations” benefit
See the “Spinal and
extremity
manipulations”
benefit on page 70
Diagnostic tests,
laboratory, and x-
rays
Standard rate
48, 61, 106-116
Durable medical
equipment (DME),
supplies, and
prostheses
Standard rate
48, 108, 111, 173
Emergency room (ER)
Special rate:
ER services are paid at the network rate at preferred,
participating and out-of- network hospitals.
You pay 15% of the allowed amount. You are usually
billed separately for:
• Facility charges
• Professional (physician) services
• Lab tests, x-rays, and other imaging tests
51, 174
Hearing aids
Special rate:
• Subject to the deductible
• You pay $0 of the $3,000 benefit limit per ear every 3
years.
54
Home health care
Standard rate
54, 109, 177, 179
Hospice care
Special rate:
• You pay $0 for medical services after meeting your
deductible
• You pay $0 for prescription drugs after meeting your
deductible
• You pay $0 for end-of-life counseling while in
hospice after meeting your deductible
54, 177
38 2024 UMP CDHP (PEBB) Certificate of Coverage
Benefit/service
How much you will pay
For information,
see page(s):
Hospital services
Inpatient rate
Outpatient/professional services: Standard rate
56, 63, 109
Mammograms
Diagnostic: Standard rate
Screening: Preventive rate
61
Mental health
See the “Behavioral health” benefit
41, 110, 112
Naturopathic
physician services
Standard rate
19, 62, 102, 107
Obstetric and
newborn care
Inpatient rate
Outpatient/professional services: Standard rate
63, 112
Office visits
Standard rate
64, 111
Prescription drugs
See the “What you pay for prescription drugs” section
90
Preventive care and
immunizations
Preventive care: Preventive rate
Covered preventive immunizations: Preventive rate
61, 64, 65, 91, 186
Skilled nursing
facility
Inpatient rate
Some services may be billed separately, such as
physical therapy
69, 109, 113, 190
Spinal and extremity
manipulations
See the “Spinal and extremity manipulations” benefit
70
Substance use
disorder
See the “Behavioral health” benefit
41
Surgery
Standard rate
56, 58, 62,65, 70,
70, 73, 77, 109, 114,
170,183 , 188
Therapy: Habilitative
and Rehabilitative
Inpatient rate
Outpatient/professional services: Standard rate
74
Tobacco cessation
Preventive rate
75
Vision care exam
(routine)
Preventive rate
81, 84
Vision hardware,
adults (age 19 or
older)
(Lenses, frames, or
contact lenses)
Special rate:
• No medical deductible
• Lenses and frames: You pay $0 of the allowed
amount for one pair of covered standard lenses and
frames once every two calendar years; or
• Contact lenses: Plan pays up to $150 every two
calendar years in lieu of lenses and frames. You pay a
$30 fitting fee for contact lenses.
81
2024 UMP CDHP (PEBB) Certificate of Coverage 39
Benefit/service
How much you will pay
For information,
see page(s):
Vision hardware,
children (under age
19)
(Lenses, frames, or
contact lenses)
Special rate:
• No medical deductible.
• Lenses and frames: You pay $0 of the allowed
amount for one pair of covered standard frames and
lenses once per year; or
• Contact lenses: You pay $0 of the allowed amount
for a one-year supply in lieu of lenses and frames.
There is no fitting fee.
85
Note: For services requiring preauthorization or plan notification, see the list of services on the UMP
Policies that affect your care webpage or contact UMP Customer Service (see Directory for link and
contact information). Many services require both preauthorization and plan notification. See the “Limits on
plan coverage” section for how this works.
List of benefits
Acupuncture
The plan covers up to 24 visits for acupuncture treatment per calendar year (see definition of “Limited
benefit”). You pay the special rate (a $15 copay) for acupuncture when you see a preferred provider after
you meet your deductible. The copay will apply toward the out-of-pocket limit. All visits apply to the 24-
visit limit.
You may receive an office visit at the time of the acupuncture service (see the “Office visits” benefit for
details). Not all acupuncture services are covered. See the “What the plan does not cover” section for
more information.
Note: For participating providers and out-of-network providers, services are paid at the standard rate up
to 24 visits per calendar year.
Ambulance
Ambulance services for personal or convenience purposes are not covered.
Ground ambulance
You pay 20 percent of the allowed amount for medically necessary ambulance services. Professional
ground ambulance services are covered in a medical emergency:
• From the site of the medical emergency to the nearest facility equipped to treat the medical
emergency.
• From one facility to the nearest other facility equipped to provide treatment for your condition.
When other means of transportation are considered unsafe due to your medical condition, the plan
covers professional ambulance services:
• From one facility to another facility, for inpatient or outpatient treatment;
• From home to a facility; or
• From a facility to home.

40 2024 UMP CDHP (PEBB) Certificate of Coverage
Air ambulance
You pay 20 percent of the allowed amount for medically necessary ambulance services regardless of
network status. You may not be balance billed. Air professional ambulance services are covered only when
all the following conditions are met:
• Ground ambulance is not appropriate
• The situation is a medical emergency
• Air ambulance is medically necessary
• Transport is to the nearest facility able to provide the care you need
ALERT! The plan will not pay for air ambulance or other forms of air transport to move you to
a facility closer to your home. If you travel outside the U.S., consider getting separate insurance
that covers such air ambulance services.
Water ambulance
You pay 20 percent of the allowed amount for medically necessary ambulance services. Water
professional ambulance services are covered only when all the following conditions are met:
• Ground ambulance is not appropriate
• The situation is a medical emergency
• Water ambulance is medically necessary
• Transport is to the nearest facility able to provide the care you need
Applied Behavior Analysis (ABA) Therapy
The plan covers Applied Behavior Analysis (ABA) Therapy only for a diagnosis of autism spectrum
disorder. Providers of ABA Therapy services must be appropriately credentialed and qualified to prescribe
or perform ABA Therapy services.
The plan must preauthorize ABA Therapy services for members age 18 years old or older before services
are performed. No preauthorization is required for members under age 18. Like other preauthorized
services, approved ABA preauthorization is specific to the provider who made the ABA preauthorization
request. ABA Therapy hours preauthorized for one provider are not automatically transferable to another
provider. A change in the provider requires a new ABA preauthorization. The initial assessment and ABA
therapy treatment order or prescription do not require preauthorization for members of any age.
As for other covered services, you receive the highest-level benefit by using preferred providers. See the
“Types of services” section for differences in your cost for preferred, participating, and out-of-network
providers. To find a preferred provider, visit the UMP Provider search or contact UMP Customer Service.
You can also find more information on ABA Therapy by viewing the ABA policy on the UMP Policies that
affect your care webpage. See the Directory pages at the beginning of this booklet for links and contact
information.
Autism treatment
To determine how a service, supply, or intervention is covered, see that specific benefit. For example,
Applied Behavior Analysis (ABA) Therapy is addressed on page 40; speech or occupational therapy is
addressed on page 74 under the “Therapy: Habilitative and Rehabilitative” benefit; and mental health
coverage is found under “Behavioral health” on page 41. If a specific benefit is subject to limits, such as

2024 UMP CDHP (PEBB) Certificate of Coverage 41
number of visits, these limits do not apply when the services, supplies, or interventions are for an autism
diagnosis.
Bariatric surgery
TIP: Contact UMP Customer Service to locate a provider.
For the plan to cover bariatric surgery, you must get preauthorization from the plan and follow all your
chosen facility’s bariatric surgery requirements. This includes working with a multidisciplinary bariatric
surgery team and ensuring your surgery and postsurgical treatment meet all plan medical policies.
The plan covers only certain types of bariatric surgery procedures. If you meet the plan’s clinical criteria,
non-Medicare adults age 18 or older will be eligible for covered bariatric procedures.
Related care following bariatric surgery
Panniculectomy (removal of loose skin) is covered following bariatric surgery when specific medical
criteria are met. Most panniculectomies are considered cosmetic and are not covered.
UMP will cover medically necessary surgical follow-up care related to a covered bariatric procedure, such
as care for complications and needed revisions. The follow-up surgery must be appropriate and essential
to the long-term success of the initial bariatric surgery and must be preauthorized.
Members who had a bariatric procedure before coverage under a UMP plan and have complications or
need medically necessary revision are not required to verify prior coverage or that they met the plan’s
medical policy criteria for the initial bariatric procedure. However, you must follow plan requirements for
follow-up care, including requesting preauthorization.
Behavioral health
The plan covers behavioral health services including care for mental health and substance use disorder.
You pay the inpatient rate when admitted to an inpatient facility, and the standard rate for all other care
and services.
When you receive nonemergency services from an out-of-network provider at a network hospital, network
hospital outpatient department, network critical access hospital, or network ambulatory surgical center,
you pay the network rate and cannot be balance billed for services performed in Washington State or
without your informed consent in states that allow you to waive the federal balance billing protections.
When you receive emergency services you pay the network cost-sharing amount regardless of the
network status of the provider or facility and cannot be balance billed.
Mental health
The plan covers mental health services for members with neuropsychiatric and mental health conditions.
Marriage or family counseling is not covered. The amount the plan pays depends on the provider’s
network status (see the “Finding a health care provider” section). See below for details about coverage for
substance use disorder treatment.

42 2024 UMP CDHP (PEBB) Certificate of Coverage
Inpatient
ALERT! Your provider must notify the plan as soon as possible after you are admitted to a
facility, but not later than 24 hours after you are admitted when you receive inpatient services.
If the plan is not notified of inpatient treatment, the plan may not cover the treatment.
Inpatient treatment is subject to clinical review.
Services are considered inpatient when you are admitted to a facility. This may include either psychiatric
inpatient hospitalization or care at a residential treatment facility. The plan must preauthorize non-
emergency inpatient services. See the “Limits on plan coverage” section for details.
Your provider must notify the plan as soon as possible after you are admitted to a facility, but no later
than 24 hours after you are admitted to a:
• Hospital
• Residential treatment facility
Contact UMP Customer Service about preauthorization requirements. Visit UMP Policies that affect your
care webpage for a list of services that require plan notice. See Directory for link and contact information.
Professional services (for example, doctors) may be billed separately from the facility charges. The plan
pays the inpatient rate unless it is for emergency services. All covered professional services are paid based
on the allowed amount.
Outpatient
ALERT! See page 40 for preauthorization requirements related to Applied Behavior Analysis
(ABA) Therapy services.
You pay the standard rate for outpatient mental health services. You pay based on the allowed amount
and the network status of the provider. Most outpatient mental health services do not require
preauthorization. Visit the UMP Policies that affect your care webpage for a list of services that require
plan notice.
Your provider must notify the plan as soon as possible, but not later than 24 hours after the following
services are initiated:
• Intensive Outpatient Therapy
• Partial Hospitalization Program (PHP)
Substance use disorder
Substance use disorder is defined as an illness characterized by a physiological or psychological
dependency on a controlled substance or alcohol. Substance use disorder does not include dependence
on tobacco, caffeine, or food.
To be covered, treatment programs must be licensed to provide treatment to persons requiring substance
use disorder treatment. The amount the plan pays depends on the provider’s network status (see the
“Finding a health care provider” section). See above for details about coverage for mental health services.
Contact UMP Customer Service about preauthorization requirements.

2024 UMP CDHP (PEBB) Certificate of Coverage 43
Inpatient
ALERT! Your provider must notify the plan as soon as possible after you are admitted to a
facility, but not later than 24 hours after you are admitted when you receive inpatient services
for substance use disorder treatment. If the plan is not notified of inpatient treatment, the plan
may not cover the treatment. Inpatient treatment is subject to clinical review.
Professional services (for example, doctors or lab tests) may be billed separately from the facility charges.
The plan pays for these services according to the network status of the provider, unless it is for emergency
services.
Your provider must notify the plan when:
• You receive detoxification services
• You are admitted to a hospital
• You are admitted to a residential treatment facility
Outpatient
You pay the standard rate for outpatient substance use disorder treatment. You pay based on the allowed
amount and the network status of the provider.
Your provider must notify the plan when you receive the following services:
• Detoxification
• Intensive Outpatient Program (IOP)
• Partial Hospitalization Program (PHP)
Preauthorization for outpatient substance use disorder treatment is not required in most cases. The plan
may require that your provider submit a treatment plan to determine medical necessity.
Behavioral health support resources
UMP provides behavioral health support resources to meet your needs.
myStrength
myStrength is a self-guided health and resiliency online tool clinically proven to improve emotional
health. This secure resource is available 24 hours a day, 7 days a week to members age 13 or older at no
cost to you. myStrength’s interactive and activity-based tools are personalized to you and address
conditions such as depression, anxiety, stress, substance use disorders, and chronic pain. Visit the
myStrength website at hca.wa.gov/ump-pebb-mystrength to sign up and learn more.
Quartet
Quartet can help match you to in-person and telemedicine behavioral health providers who are in the
plan’s network and offer an array of behavioral health services, including, but not limited to, mental health
counseling, substance use disorder, and psychiatry services. You pay the standard rate for behavioral
health services. Get started by visiting Quartet’s website at qrt.care/pebb-network-providers or by calling
Quartet’s Care Navigation Team at (253) 248-6588 (TRS: 711).
Note: Quartet is only available to UMP members age 18 or older who reside and are seeking care in
Washington State.
44 2024 UMP CDHP (PEBB) Certificate of Coverage
Breast health screening tests
See also the “Mammogram and Digital Breast Tomosynthesis (DBT)” benefit for more information about
breast health screening tests. The tests listed below may be covered for diagnostic purposes as indicated
under plan medical policy.
Services covered
• Members age 40 or older: Breast health screening tests, as well as digital mammograms, are covered
as preventive.
• Members under age 40: See the “Mammogram and Digital Breast Tomosynthesis (DBT)” benefit for
how preventive breast health screening tests are covered for high-risk members.
Services not covered
The procedures listed below are not covered by the plan when they are performed supplementary to
digital mammography for screening purposes for members with or without dense breasts.
Non-high-risk members:
• Automated Breast Ultrasound (ABUS)
• Handheld Ultrasound (HHUS)
• Magnetic Resonance Imaging (MRI)
High-risk members:
• Automated Breast Ultrasound (ABUS)
• Handheld Ultrasound (HHUS)
Care Gap Closure Program
The Care Gap Closure Program encourages members to receive recommended preventive and chronic
care services and screenings, also known as “gaps in care.” These include screenings for cancer, diabetes,
and more at no cost to you. This support includes helping members find a PCP, making appointments,
ensuring members understand their benefits, and providing members ongoing support through case
management, as needed. Contact UMP Customer Service for more information.
Care management
Regence care management supports the unique needs of members with chronic, serious, or sudden
illness or injury and prioritizes those needs by providing personalized services that enhance well-being.
Care management teams can help with:
• Advocating for members and their support systems and improving care through close collaboration
with providers.
• Assisting members as they navigate the health care system, including helping members find preferred
providers and facilities, and supporting members transitioning to different levels of care.
• Educating members about their care options, benefits, and coverage, as well as helping members make
educated decisions regarding their health care.
• Supporting members with coordination of care needs.
We offer a single-nurse model dedicated to delivering personalized and holistic medical and behavioral
health support to each member and their family. Once a member is engaged in the care management
program, they may be assigned a case manager who is a licensed social worker or registered nurse.
Regence case managers work closely with a member and their providers to help meet treatment plan
goals and improve a member’s overall health.

2024 UMP CDHP (PEBB) Certificate of Coverage 45
How to get started
Providers may refer members, and Regence also proactively reaches out to members most likely to
benefit from care management support. Members can also self-refer by calling Regence at 1-866-543-
5765 (TRS: 711) for information about care management services.
What’s next
Once a member is identified for care management, the designated case manager calls the member. The
Regence case manager will attempt at least three calls and will send a letter to the member. The member
can respond to the letter if they wish to engage with a case manager. Providers are sent a letter or
contacted by phone when their patient is enrolled in care management.
Care management newsletters
Newsletters are sent once per year with an option to opt into care management to all members with a
new diagnosis of depression, anxiety, a painful condition, or adult/pediatric cancer.
Condition-specific newsletters are sent twice per year with an option to opt into care management to all
members diagnosed with coronary artery disease (CAD), congestive heart failure (CHF), chronic
obstructive pulmonary disease (COPD), asthma, or diabetes.
Case management as a condition of coverage
An HCA or plan medical director may review medical records and determine that your use of certain
services is potentially harmful, excessive, or medically inappropriate. Based on this determination, the plan
may require you to participate in and comply with a case management plan as a condition of continued
benefit payment.
Chiropractic physician services
See the “Spinal and extremity manipulations” benefit.
Dental services
ALERT! Dentists and other dental providers are not included in the UMP provider network,
even if they are listed in the Regence provider directory.
The plan does not cover most dental services. For example, dental implants, orthodontic services, and
treatment for damage to teeth or gums caused by biting, chewing, grinding, or any combination of these
are not covered. However, your PEBB dental plan may cover these services. Refer to your dental plan’s
COC, found on the HCA website at hca.wa.gov/erb, for more information.
What is covered by the plan
The plan covers oral surgery and other dental services under the medical benefit when they are
considered medical. Oral surgery and dental services are considered medical if the condition being
diagnosed and treated is either one which is not connected to the teeth and/or gums or is related to a
disease or illness that affects the whole body. These medical services may be performed by a dentist or
medical professional provider. You can find examples of these medical services in the Regence Medical
Policy Administrative Guidelines to Determine Dental vs Medical Services by visiting the UMP Policies that
affect your care webpage (see Directory for link). You pay 20 percent of the allowed amount for covered
dental services unless otherwise stated, and the provider may balance bill you.

46 2024 UMP CDHP (PEBB) Certificate of Coverage
Note: UMP is not affiliated with the Uniform Dental Plan (UDP). If you are enrolled in UDP, contact UDP
for information about services covered under your dental plan. Visit the HCA website at hca.wa.gov/erb
and select “Contact” to find UDP contact information.
Fluoride treatment
Under certain circumstances, the plan may cover fluoride supplements (see the “Preventive care” benefit)
at the preventive rate. The application of fluoride varnish may be covered for infants and children starting
at the age when primary teeth come in (primary teeth eruption) in primary care practices for prevention of
tooth decay (dental caries or cavities). Coverage of fluoride treatment depends on the network status of
the medical provider as described in the “Finding a health care provider” section. Health care providers,
such as your child’s medical PCP, may apply fluoride varnish.
General anesthesia during a dental procedure
General anesthesia performed during a dental procedure is covered only when:
• It is provided by an anesthesiologist; and
• The charges are covered by the plan (see below).
Dental procedures
General anesthesia may be performed in a dental office for covered procedures and is paid at the
standard rate. Dental procedures that are performed in a hospital or ambulatory surgery center are
covered only when the member:
• Is under age 8 with a dental condition that cannot be safely and effectively treated in a dental office; or
• Has a dental condition that cannot be safely and effectively treated in a dental office because of a
physical or developmental disability; or
• Has a medical condition that would put the member at undue risk if the procedure were performed in a
dental office.
Accidental injuries
To receive coverage for repair of an accidental injury to natural teeth, the injury must be evaluated, and a
treatment plan developed and finalized within 30 days of the injury.
The actual treatment may extend beyond 30 days if your provider determines upon the initial assessment
that treatment should start later or continue longer. Treatment must be completed by the end of the
calendar year following the accident. The plan does not cover treatment after UMP coverage ends.
Example: You have an accident on March 12, 2024, resulting in injuries that are covered by the plan. Your
treatment plan must be finalized no later than April 11, 2024. All related treatment must be completed by
December 31, 2025 (the calendar year following the accident).
The plan does not cover treatment that:
• Was not included in the treatment plan developed within the first 30 days following the accident;
• Extends past the end of the calendar year following the accident; or
• Extends past the end of your enrollment in the plan.
Diabetes care supplies
TIP: If a health plan other than UMP is your primary payer, claims for diabetes care supplies
may be paid differently (see page 120).

2024 UMP CDHP (PEBB) Certificate of Coverage 47
Medical
Insulin pumps and pump supplies are covered as durable medical equipment (DME). See page 50 for
coverage of insulin pumps and related supplies.
Prescription drug
Diabetes care supplies listed below are only covered under your plan’s prescription drug benefit:
• Insulin syringes
• Lancets
• Test strips
• Continuous glucose monitors
To be covered, you must get a written prescription for these supplies and purchase them from a
pharmacy. Limits, such as quantity limits or preauthorization, may apply. For questions, contact WSRxS
Customer Service.
You save money and avoid having to submit your own claims when you purchase these diabetes care
supplies from a WSRxS network pharmacy. Locate a network pharmacy by visiting the UMP Prescription
drug coverage webpage or contact WSRxS Customer Service (see Directory for link and contact
information).
For more information, see “Exceptions covered" on page 91.
Diabetes Control Program
TIP: The Diabetes Control Program is not subject to your deductible and is offered at no
additional cost for UMP (non-Medicare) members age 18 or older.
For non-Medicare members age 18 or older with a diagnosis of diabetes, the plan offers the Diabetes
Control Program administered by the Care Management Program at Regence. Case managers are trained
to help you reduce the risk of complications of diabetes by tracking and controlling blood sugar,
cholesterol levels, blood pressure, and weight in a series of quarterly consultations. The plan offers the
Diabetes Control Program at no additional cost to members.
You may find out if you have diabetes by visiting your primary care provider for a blood sugar laboratory
test. If you qualify for the Diabetes Control Program, you may self-refer by calling Regence at 1-866-543-
5765 (TRS: 711).
Diabetes education
The plan covers diabetes self-management training and education, including nutritional therapy by
registered dieticians. When diabetes education includes nutritional therapy, the nutritional therapy
services are not subject to the 12-visit lifetime limit stated under “Nutrition counseling and therapy” on
page 62.
Diabetes Prevention Program (DPP)
You may be eligible for DPP if:
• You are not a Medicare member;
• You are age 18 and older;
48 2024 UMP CDHP (PEBB) Certificate of Coverage
• Your provider ordered a blood sugar test in the last 12 months; and
• Laboratory results showed you are in the prediabetes range
DPP provides access to a virtual (online) program through Omada Health.
You may take an online screening questionnaire to see if you meet the program’s criteria by visiting the
DPP website at go.omadahealth.com/wapebb, creating an account, and signing in. If you meet the
criteria, you may participate in the program at no cost to you. The virtual program includes a professional
health coach, a wireless scale, and weekly online classes with a small group of participants who provide
real-time support. You may also contact UMP Customer Service for more information.
Diagnostic tests, laboratory, and x-rays
You pay the standard rate for covered diagnostic tests, laboratory tests, and x-rays when medically
necessary. If there are alternative diagnostic approaches with different fees, the plan will cover the least
expensive, evidence-based diagnostic method. Visit the UMP Policies that affect your care webpage or
contact UMP Customer Service for a list of services requiring preauthorization (see Directory for link and
contact information).
Covered services include:
• All prostate cancer screening (prostate-specific antigen [PSA testing]), which is subject to your
deductible and coinsurance, even if billed as preventive.
• Colonoscopy performed to diagnose disease or illness. See the list on page 65 for coverage of
preventive or screening colonoscopy.
• Diagnostic laboratory tests, x-rays (including diagnostic mammograms), and other imaging studies.
• Electrocardiograms (EKG, ECG).
• Skin allergy testing.
TIP: See page 61 to learn how the plan covers mammograms.
The plan does not pay for the following tests (this list does not include all tests not covered by the plan):
• Carotid Intima Media Thickness testing.
• Computed Tomographic Colonography (CTC) (also called a virtual colonoscopy) for routine screening.
• Upright Magnetic Resonance Imaging (uMRI), also known as “positional,” “weight-bearing” (partial or
full), or “axial loading.”
Dialysis
You pay the standard rate for covered dialysis services. The plan pays based on the allowed amount and
the network status of the provider. Other professional providers may bill separately from the facility.
Durable medical equipment (DME), supplies, and prostheses
TIP: The plan pays for covered DME at the standard rate. To receive the highest benefit, you
must get the equipment or supply from a preferred DME supplier or other preferred medical
provider. To find preferred DME providers, see the “Finding a preferred DME supplier” section
below.
2024 UMP CDHP (PEBB) Certificate of Coverage 49
You pay the standard rate for covered DME services and supplies if they are prescribed by a provider
practicing within their scope of practice, medically necessary, and used to treat a covered condition,
including, but not limited to:
• Artificial limbs or eyes (including implant lenses prescribed by a physician and required due to cataract
surgery or to replace a missing portion of the eye).
• Automatic Positive Airway Pressure (APAP) devices and related supplies.
• Bi-level Positive Airway Pressure (BiPAP) devices and related supplies.
• Bone growth (osteogenic) stimulators.
• Breast prostheses and bras as required by mastectomy. See the “Mastectomy and breast
reconstruction” benefit.
• Breast pumps for pregnant and nursing members (see “Services covered as preventive” on page 64).
• Casts, splints, crutches, trusses, and braces.
• Compression stockings.
• Continuous Positive Airway Pressure (CPAP) devices and related supplies.
• Diabetic shoes, only as prescribed for a diagnosis of diabetes. See the “Foot orthotics” section below.
• Elemental formulas for Eosinophilic Gastrointestinal Disorders (EGIDs).
• Insulin pumps and related pump supplies (see the “Insulin pumps and related pump supplies” section
below).
• Ostomy supplies.
• Oxygen and its equipment, such as all types of concentrators and tanks for administration, are covered
on a rental basis only.
• Penile prosthesis when other accepted treatment has been unsuccessful and impotence is:
▪ Caused by a covered medical condition; or
▪ A complication directly resulting from a covered surgery; or
▪ A result of an injury to the genitalia or spinal cord.
• Rental or purchase (at the plan's discretion) of DME such as wheelchairs, hospital beds, and respiratory
equipment. (The combined rental fees cannot exceed full purchase price.)
• Wig or hairpiece to replace hair loss due to radiation therapy or chemotherapy for a covered condition,
up to a lifetime maximum of $100. Wigs and hairpieces for any other reason are not covered.
Some items require preauthorization. Find the list of supplies that require a preauthorization by visiting
forms and publications at hca.wa.gov/ump-forms-pubs and search “durable medical equipment” or
contact UMP Customer Service.
The plan limits coverage of DME to one item of a particular type of equipment and the accessories
needed to operate the item. If you receive a higher-cost DME item when a less expensive, medically
appropriate option is available, the plan will not pay for the more expensive item.
The plan also covers the repair or replacement of DME due to normal use or a change in the member’s
condition (including the growth of a child). You are responsible for the entire cost of any additional pieces
of the same or similar DME you purchase or rent for personal convenience or mobility.
Note: The plan does not cover replacement of lost, stolen, expired, or damaged DME.

50 2024 UMP CDHP (PEBB) Certificate of Coverage
Foot orthotics
Items such as shoe inserts, foot orthotics, and other shoe modifications are covered only when both of
these conditions are met:
• The member has been diagnosed with diabetes.
• Specialized (including customized) orthotics are prescribed to treat or reduce the risk of diabetes
complications.
If you have questions about what services are covered, contact UMP Customer Service.
Insulin pumps and related pump supplies
Insulin pumps and related pump supplies are covered as DME. For the highest benefit level, use a
preferred DME supplier.
ALERT: Continuous glucose monitors are not covered under the DME benefit. They are
covered under the prescription drug benefit. See the “Diabetes care supplies” benefit for more
information.
Finding a preferred DME supplier
You may purchase DME through a medical supplier. To find a preferred DME supplier, visit the UMP
Provider search (see Directory for link). You do not have to sign in to the Regence member site to search
for a provider, but you will get more personalized results if you do. Click on the “All categories” link
(found beneath “Doctors by name” and “Doctors by specialty”). Type “durable medical” into the search
box; a drop-down list will appear. Select “Durable Medical Equipment & Supplies.” You should now have a
list of network DME suppliers. Preferred providers are paid at the highest rate and are noted as a Category
1 provider in the UMP provider search. Different DME suppliers carry different types of supplies. You may
need to call to confirm that a supplier has what you need.
Commercial DME
You may purchase DME on Amazon by signing in to your Regence account and going to the Regence
medical supplies webpage at regence.com/member/medical-supplies/. Select “Get started” in the Shop
smart and save section. This will take you to the Amazon page where you will select and shop from one of
the four categories for DME supplies:
• Post-mastectomy
• Illness and injury
• New parents
• Manage a condition
You pay 100 percent of the billed charge and submit a claim for reimbursement. To submit a claim, select
“Start your claim” in the “How to get repaid” section on the Regence medical supplies webpage at
regence.com/member/medical-supplies/. The plan will reimburse you 85 percent of the allowed amount
for covered DME supplies purchased through Amazon. To learn more contact UMP Customer Service.
2024 UMP CDHP (PEBB) Certificate of Coverage 51
Emergency room
TIP: If you need immediate care but your situation is not a medical emergency, see the “Urgent
care” benefit for how to get treatment at a lower cost than in an emergency room.
The plan covers facility charges for emergency room treatment when the treatment is for covered
diagnoses and treatment of an injury. Covered services are paid at 85 percent of the allowed amount after
you pay your deductible.
Charges for professional services may be billed separately from facility (hospital or emergency room)
charges. When you receive emergency services, you cannot be balance billed.
If your emergency room visit is determined to be a medical emergency, it will be paid at the network rate
for preferred, participating, and out-of-network facilities. Separate professional services charges will also
be paid at the network rate if your emergency room visit is determined to be a medical emergency.
End-of-life counseling
End-of-life counseling involves discussing and planning for your end-of-life care, including treatment
options and advanced directives. The plan covers end-of-life counseling for all members up to 30 visits
per year. There is no requirement to be terminally ill, on hospice, or in the final stages of life to receive
end-of-life counseling services. End-of-life counseling associated with hospice services is paid at 100
percent after you meet your deductible. Outside of hospice, these services are paid as a medical benefit,
subject to your deductible and coinsurance. For more information on hospice care, see page 55.
Family planning services
If you receive care from a network provider, the plan will pay for the following covered services at 100
percent after you meet your deductible:
• Contraceptive drugs and devices including condoms and spermicides
• Voluntary and involuntary termination of pregnancy (abortion or miscarriage)
• Education and counseling related to contraception
If you receive care from an out-of-network provider, covered services are paid at the standard rate and
the provider may balance bill you. If you go to a non-network pharmacy, you may have to pay at the time
of purchase and submit a claim for reimbursement (see the "Submitting a claim for prescription drugs"
section). You must get over-the-counter contraceptive supplies from a network pharmacy for these items
to be covered (see “Over-the-counter contraceptives” in the next section below). Prescriptions purchased
from an excluded pharmacy will not be covered. See the definition of “Excluded pharmacy.”
Contraceptives
ALERT! Visits for placement and removal of covered contraceptive devices that require
professional insertion and removal are covered at the preventive rate.
Contraceptives are covered under the prescription drug benefit. Contraceptives include, but are not
limited to, birth control pills, emergency contraception (the “morning after” pill), vaginal rings, patches,
52 2024 UMP CDHP (PEBB) Certificate of Coverage
implants, injectables, condoms, and spermicides. Final determination of medical necessity for FDA
approved contraceptives is determined by the prescribing provider. Quantity limits still apply.
You may purchase up to a 12-month supply of contraceptives. Contact Washington State Rx Services
(WSRxS) Customer Service for information on how to obtain a 12-month supply. The replacement of lost,
expired, or stolen contraceptives is not covered.
You may obtain emergency contraception over-the-counter without a prescription. When possible, it is
best to obtain a prescription, since not all pharmacies have prescribing authority. If you go to a pharmacy
without a prescription and the pharmacy does not have prescribing authority, you will need to submit a
claim to WSRxS. Members will need to contact the pharmacy directly for information on prescribing
authority.
Barrier devices
All barrier devices requiring a prescription, fitting, insertion (includes IUD placement immediately after
delivery), or removal are paid at the preventive rate when you see a preferred or participating provider or
use a network pharmacy. Barrier devices requiring a prescription or fitting include intrauterine devices
(IUDs), diaphragms, and cervical caps.
Over-the-counter contraceptives
Over-the-counter contraceptives are covered under the Preventive Tier (P) on the UMP Preferred Drug List
(see “The UMP Preferred Drug List” section for more information), only if they are approved by and
registered with the FDA.
For the plan to cover FDA-registered over-the-counter contraceptives, you must present your UMP
member ID card and make your purchase at the pharmacy counter. When possible, it is best to obtain a
prescription, since not all pharmacies have prescribing authority. If you go to a pharmacy without a
prescription and the pharmacy does not have prescribing authority, you will need to submit a claim to
WSRxS.
Sterilization
When you see a preferred provider, sterilization procedures, such as tubal ligation or vasectomy, are
covered as follows:
• For females: Covered as preventive (not subject to your deductible and the plan pays 100 percent of
the allowed amount).
• For males: Paid at 100 percent after you meet your deductible.
Services and products not covered under the family planning benefit
The plan does not cover the following services and products as a family planning benefit:
• Over-the-counter products not approved by and registered with the FDA
• Reversal of voluntary sterilization
• Treatment of fertility or infertility, including direct complications resulting from such treatment
Foot care, maintenance
Maintenance foot care includes services such as toenail trimming and corn or callous removal or
trimming. These services are covered only for a diagnosis of diabetes and when provided by an approved
provider type. The plan does not cover maintenance foot care provided outside the diagnosis of diabetes.
Gender affirming care
With a diagnosis of gender dysphoria, the following services are covered at the standard rate for
outpatient services and at the inpatient rate for inpatient services:

2024 UMP CDHP (PEBB) Certificate of Coverage 53
• Covered surgical services
• Non-surgical services, including, but not limited to, hormone therapy, office visits, mental health
counseling, and tests
This is not a complete list of medical and surgical treatments of gender dysphoria in transgender
individuals. For more information on gender affirming care, visit the UMP Policies that affect your care
webpage (see Directory for link) to find the clinical criteria for gender affirming care. Some services and
prescription drugs associated with gender dysphoria may require preauthorization.
Genetic services
Covered genetic tests require preauthorization. With preauthorization, the plan covers medically
necessary, evidence-based genetic testing services. Some genetics tests are not covered. For information
about genetic services related to the fetus during pregnancy, see “Services for obstetric and newborn
care” on page 63. Contact UMP Customer Service with any questions.
Headaches, chronic migraine or chronic tension type
The plan only covers the treatment of chronic migraine with OnabotulinumtoxinA (Botox) when both the
following criteria are met:
• The condition has not responded to at least three prior pharmacological prophylaxis therapies from
two different classes of prescription drugs; and
• The condition is appropriately managed for medication overuse.
Botox injections must be discontinued when:
• The condition has shown inadequate response to treatment (defined as less than 50 percent reduction
in headache days per month after two treatment cycles); or
• The member has received a maximum of five treatment cycles.
The following treatments are not covered:
• Treatment of chronic tension-type headaches with Botox or acupuncture; and
• Treatment of chronic migraine or chronic tension-type headaches with massage, trigger point
injections, transcranial magnetic stimulation, or manipulation/manual therapy (such as chiropractic
services).
Hearing care (diseases and disorders of the ear)
The plan pays under the medical benefit for covered services for treatment of diseases and disorders of
the ear or auditory canal not related to routine hearing loss. These services are not part of “Hearing exam
(routine)” and “Hearing aids” below.
Hearing exam (routine)
ALERT! The plan pays for a hearing exam performed as part of a newborn screening at the
preventive rate.
You pay the standard rate for one routine hearing exam per calendar year.

54 2024 UMP CDHP (PEBB) Certificate of Coverage
Hearing aids
You pay $0 of the $3,000 benefit limit per ear every 3 calendar years once you have met your deductible
for prescribed hearing aids. You are responsible for hearing aid charges exceeding the $3,000 benefit
limit. See the definition of “Limited Benefit”.
You pay the standard rate for the following hearing-related services:
▪ Ear mold(s)
▪ Initial battery, cords, and other ancillary equipment
▪ Warranty (only as included with the initial purchase)
▪ Follow-up consultation within 30 days after delivery of hearing aid
▪ Rental charges up to 30 days if you return the rented hearing aid before actual purchase
▪ Repair of hearing aid equipment
▪ The initial assessment, fitting, adjustment, auditory training, and other ear molds as necessary to
maintain an optimal fit for those who have obtained or intend to obtain a hearing aid
The following hearing-related items are not covered:
• Over-the-counter hearing aids that are not prescribed, except for initial assessment, fitting, adjustment,
auditory training, and ear molds as necessary to maintain an optimal fit
• Charges incurred after your plan coverage ends, unless you ordered the hearing aid before that date
and it is delivered within 45 days after your coverage ended
• Extended warranties, or warranties not related to the initial purchase of the hearing aid(s)
• Purchase of replacement batteries or other ancillary equipment, except those covered under terms of
the initial hearing aid purchase
The following ancillary equipment is not covered:
• Alerting devices
• Assistive listening devices for FM/DM systems, receivers and transmitters
• Assistive listening devices for microphone transmitters
• Assistive listening devices for TDD machines
• Assistive listening devices for telephones
• Assistive listening devices for televisions (including amplifiers and caption decoders)
• Assistive listening devices for use with cochlear implants
• Assistive listening devices, supplies, and accessories not otherwise specified
• Hearing aid batteries
Home health care
ALERT! See the “What the plan does not cover” section for services the plan does not cover.
In certain circumstances, the plan covers short-term, provider-directed, medically necessary home health
services on an intermittent or part-time basis by a licensed home health, hospice, or home care agency, to
2024 UMP CDHP (PEBB) Certificate of Coverage 55
help a member recover from an acute covered illness, injury, or hospital stay. Home Health care is
provided through visits from specialized clinicians, performing specific tasks (rather than time-based
shifts), on a short-term basis, until specified individual goals are met. These services must be part of a
treatment plan written by your provider (such as your physician or advanced registered practitioner
[ARNP]). The provider must certify that you are homebound. These short-term visits may include:
• Skilled nursing care, physical, occupational, or speech therapy
• Home health aides and clinical social services, provided in conjunction with the skilled services of a
registered nurse (RN), licensed practical nurse (LPN) or physical, occupational, or speech therapist
• Disposable medical supplies as well as prescription drugs provided by the home health agency
• Home infusion therapy
• Home care of wounds resulting from injury or surgery
• End-of-life counseling (see page 51)
For services that may be covered under another benefit, such as nutritional counseling or follow-up care
for bariatric surgery, see that benefit in this COC for coverage rules and limitations. These limitations
apply even if the services are provided in the home or by a home health provider. For information on
substitution of private duty nursing as an alternative benefit in lieu of hospitalization or in lieu of
admission to a skilled nursing facility, see page 57 (hospital services) or page 69 (skilled nursing facility).
Contact UMP Customer Service if you have questions.
Hospice care
Hospice (inpatient, outpatient, and respite care) is services provided by a state-licensed hospice program
in the home or in a hospice facility to terminally ill patients. Services include pain relief care and support
services that address the needs of terminally ill members and their families without intent to cure.
Medical
Hospice services received from preferred and participating providers are covered at 100 percent of the
allowed amount after you meet your deductible. The plan covers hospice care for terminally ill members
for no more than six months. See page 51 for coverage of end-of-life counseling.
If you need hospice care, your provider will refer you to the program. For additional assistance, you may
contact UMP Customer Service.
Prescription drugs
For covered prescription drugs, UMP members in hospice care receive special coverage when using
network pharmacies, including the network specialty drug pharmacy and the network mail-order
pharmacies.
• Until your deductible is met, the member pays the full cost (allowed amount at a network pharmacy)
for covered prescription drugs, except for covered insulins. There is no deductible for covered insulins.
• After you pay your deductible, the plan pays for all covered prescription drugs purchased through a
network pharmacy at 100 percent of the allowed amount for members in hospice care.
This applies only to the member in hospice care.
All quantity limits, preauthorization requirements, and coverage limits apply.
56 2024 UMP CDHP (PEBB) Certificate of Coverage
ALERT! The member pays the full cost for noncovered prescription drugs. If the member
purchases covered prescription drugs from a non-network pharmacy, the plan pays under the
normal prescription drug benefit as described in the “What you pay for prescription drugs”
section. Prescriptions purchased from an excluded pharmacy will not be covered. See the
definition of “Excluded pharmacy.”
Respite care
Respite care is continuous care of more than four hours a day to give caretakers temporary relief from
caring for a member who is homebound or in hospice. The plan covers these services at 100 percent of
the allowed amount after you meet your deductible, up to 14 visits per the member’s lifetime.
Death with Dignity
The Washington Death with Dignity Act allows terminally ill adults seeking to end their life to request
lethal doses of prescription drugs. These terminally ill patients must be Washington residents who have
less than six months to live. For more information about this Act, see chapter 70.245 RCW.
Care described under this Act includes services covered by UMP, subject to standard plan requirements.
If you have questions about medical services UMP covers, contact UMP Customer Service. If needed, UMP
may assign a case manager to support you.
If you have questions about prescription drugs UMP covers, contact WSRxS Customer Service.
If your current provider is unable to meet your needs, or if you need assistance in finding a provider for
these services, visit End of Life Washington’s website at endoflifewa.org. End of Life Washington is a
community resource available to support the public in finding available providers.
For more information about the Death with Dignity Act, visit:
• The Department of Health’s website at
doh.wa.gov/YouandYourFamily/IllnessandDisease/DeathwithDignityAct.
• The Washington State Hospital Association’s website at wsha.org/for-patients/end-of-life/.
Hospital services
ALERT! Many services provided in a hospital setting require preauthorization, notice, or both.
Failure to request or receive preauthorization, or to notify the plan, may result in complete
denial of claims. See the “Limits on plan coverage” section for how preauthorization and notice
work.
This benefit covers hospital accommodations and inpatient, outpatient, and ambulatory care services,
supplies, equipment, and prescribed drugs to treat covered conditions. Room and board is limited to the
hospital’s average semiprivate room rate, except where a private room is determined to be medically
necessary. Some services require preauthorization. Visit the UMP Policies that affect your care webpage
for the list of these services, or contact UMP Customer Service. See Directory for link and contact
information.
If you receive a higher-cost service or device at a hospital when a less expensive, medically appropriate
option is available, you may have to pay the difference in cost. A preferred hospital cannot charge you for
2024 UMP CDHP (PEBB) Certificate of Coverage 57
the difference in cost between the standard and higher-cost item (unless you agreed in writing to pay
before receiving the services).
If benefits change under the plan while you are in the hospital (or any other facility as an inpatient),
coverage is based on the benefit in effect when the stay began.
Inpatient
Services are considered “inpatient” when you are admitted as inpatient to a hospital. Your provider must
notify the plan as soon as possible after you are admitted, but not later than 24 hours after you are
admitted. Professional services — such as lab tests, surgery, or other services — may be billed separate
from the hospital. The plan pays these services according to the network status of the provider, unless
your condition is a medical emergency (see the “Emergency room" benefit for more information). The
plan pays for all covered professional services at the standard rate.
Private duty nursing furnished by a licensed home health agency may be substituted as an alternative to
hospitalization only if:
• Inpatient hospitalization is medically necessary and would be covered by the plan;
• Private duty nursing is the most cost-effective setting (private duty nursing must be an equal or lesser
cost compared to hospitalization); and
• The member's provider agrees that private duty nursing is medically appropriate and will adequately
meet the member's needs.
Private duty nursing is shift-based, hourly nursing care at home for adults and children, typically with a
chronic illness, injury, or disability.
Substitution of private duty nursing in lieu of inpatient hospitalization has the same requirements as the
hospital benefit. For example, all deductibles and coinsurances apply.
Outpatient
Services are considered “outpatient” when you are not admitted to the hospital. Your cost depends on the
services provided, such as lab tests, and the network status of the provider(s) involved in your care. Some
services require preauthorization. Visit the UMP Policies that affect your care webpage for the list of these
services, or contact UMP Customer Service. See Directory for link and contact information.
Not all providers at a network hospital are network providers
Some providers who work in a network hospital or other network facility, including, but not limited to,
anesthesiologists and emergency room doctors, may not be network providers.
When you receive nonemergency services at a network hospital, network hospital outpatient department,
network critical access hospital, or network ambulatory surgical center in Washington State, you pay the
network rate and cannot be balance billed regardless of the network status of the provider. For
nonemergency services performed at one of these facilities outside of Washington State, you still pay the
network rate, but in some states, an out-of-network provider may be allowed to ask you to waive some of
your balance billing protections.
Infusion drug site of care program
The plan covers provider-administered infusion drugs when administered at an approved site of care.
Approved sites of care include standalone infusion sites, doctor's offices, home infusion and some
outpatient hospital facilities. Infusion drugs in the site of care program require preauthorization by the
plan before services are performed, or services will not be covered. Your provider must submit a
preauthorization request for an unapproved site of care. See the “Limits on plan coverage” section for
preauthorization instructions.
58 2024 UMP CDHP (PEBB) Certificate of Coverage
Contact UMP Customer Service for the drugs covered under the site of care program, more information,
or help finding an approved site of care near you.
Joint replacement surgery, knees and hips in the Centers of
Excellence (COE) Program
The Centers of Excellence (COE) Program covers 100 percent of the allowed amount for covered services
after you meet your deductible related to single knee or single hip total joint replacement surgery. The
program includes, but is not limited to:
• Presurgical consultations.
• Travel costs (see the “Travel benefits” section below).
• Hospitalization and surgery, if surgery is determined to be appropriate.
• Postsurgical check-ups.
In the COE program, members work with Premera Blue Cross (the administrator of the program) and
Virginia Mason Medical Center (the Center of Excellence) to make sure that their treatment is consistent
with established standards of medical care.
Premera will help you understand how the COE Program works, what is covered under the Program,
connect you with Virginia Mason Medical Center providers if you are eligible, and work to resolve any
questions or issues you may have.
If you receive services related to joint replacement that are not covered under the COE Program, but are
covered under the plan, you will pay your normal UMP cost-share, depending on the services received
and the network status of the provider(s). This may be a deductible, coinsurance, or amounts not covered
by the plan. Services billed to the plan outside of the COE Program are subject to the plan’s
preauthorization requirements.
COE for knee and hip joint replacement: Virginia Mason Medical Center
Virginia Mason Medical Center is the only provider approved to perform single knee and single hip
replacement under the COE Program. Virginia Mason Medical Center has proven that it provides high-
quality joint replacements using the most up-to-date medical guidelines and services.
Who is eligible to participate in the COE Program?
You are eligible to participate in the COE Program if you are:
• A member enrolled in UMP CDHP.
• Not enrolled in Medicare as your primary coverage.
• Age 18 or older.
How to apply to participate in the COE Program
If you are interested in participating in the COE Program:
• You may self-refer by calling Premera at 1-855-784-4563 (TRS: 711).
• Your regular provider may refer you.
You may receive information in the mail about the COE Program, which will explain how the program
works and whom to contact for more information. Premera will screen applicants to initially determine
whether they are eligible to participate in the COE Program.
What happens after you are approved to participate
After you are approved to participate in the program, Premera will:

2024 UMP CDHP (PEBB) Certificate of Coverage 59
• Provide a booklet to participants describing their journey through the program.
• Assign participants a dedicated case manager who will walk participants through each step of the
journey.
• Gather relevant medical records to supply to the participant’s COE care team as part of the referral
process. This information helps the care team assess next steps.
After Premera’s referral, Virginia Mason Medical Center will:
• Review the participant’s medical records and schedule an evaluation appointment to determine
whether the surgery is medically appropriate for the participant under the COE Program.
• Provide a list from which participants may select their surgeon if the participant is approved for
surgery.
Virginia Mason Medical Center must determine if surgery for joint replacement is appropriate based on
established medical guidelines. You may find these guidelines on the Policies that affect your care
webpage (see Directory for link).
What is included in the COE Program
In general, all eligible expenses associated with single knee or single hip replacement surgery (if
determined surgically appropriate) under the COE Program are covered. If surgery is recommended, this
includes expenses from the day you arrive for your pre-operative visit through discharge, including your:
• Assessment(s).
• Surgery.
• Hospital stay.
• Hospital discharge (excluding take-home prescription drugs, which are covered under your UMP
prescription drug benefit).
Travel benefits
Members participating in the COE Program may qualify for assistance with travel and lodging expenses.
These expenses may include partial coverage by Premera for mileage, flights, parking, and lodging.
To be covered by the program, all travel must be arranged through Premera. This travel may be
arranged by calling Premera at 1-855-784-4563 (TRS: 711).
You must have an approved adult care companion, whose travel expenses will be covered as described
below. You may be partially reimbursed for expenses related to:
• Mileage for driving within Washington. To qualify for reimbursement for mileage, members must live at
least 60 driving miles from Virginia Mason Medical Center, located at 1100 9th Ave., Seattle, WA 98101.
• Flights departing from and arriving at airports within Washington or Portland International Airport. You
must depart from the airport closest to your residence.
• Ground transportation from Seattle-Tacoma International Airport to Virginia Mason Medical Center.
• Lodging expenses (excluding meals) at a COE-designated hotel. Premera must arrange all lodging.
• Parking at Virginia Mason Medical Center and parking at your departing airport.
TIP: Reimbursement for travel expenses is based on cost or current IRS rates for medical
expenses, whichever is less, and may not cover all of your costs. For the IRS rates, visit the
IRS website at irs.gov/tax-professionals/standard-mileage-rates.

60 2024 UMP CDHP (PEBB) Certificate of Coverage
What is not included in the COE Program
If you receive services outside of the COE Program, or choose to receive services at Virginia Mason
Medical Center that are not related to your single knee or single hip replacement surgery, covered
services will be processed at the standard rate.
The following services are not included in the COE Program (but may be covered by other plan benefits):
• Care received as part of the plan Virginia Mason Medical Center gives you as a condition of surgery,
regardless of where you receive care. Examples include tobacco cessation and weight loss programs.
• Physical therapy that is not provided during your hospitalization.
• Follow-up care other than the initial postsurgical checkup at Virginia Mason Medical Center. An
example of follow-up care is a visit with your regular doctor.
• Prescription drugs received from a pharmacy after discharge from the hospital.
• Convenience items, such as a personal phone.
Contact UMP Customer Service if you have questions about services not included in the COE Program.
What happens if you are not an appropriate candidate for joint replacement
surgery under the COE program
If Virginia Mason Medical Center determines you are not an appropriate candidate for joint replacement
surgery, you may still receive joint replacement through other providers under this plan. Services received
outside the COE Program are processed according to the plan’s medical policies, benefit structure, and
the network status of your provider.
Appeals related to the COE Program
UMP members may appeal denials made by Premera. Appeals must be submitted to Premera. A decision
by your Virginia Mason Medical Center provider regarding whether the provider is willing to perform joint
replacement surgery on you is a decision of the provider, not the plan, and cannot be appealed to the
plan or Premera.
TIP: Appeal deadlines and other rules remain the same. See the “Complaint and appeal
procedures” section for details of how non-COE appeals work.
An appeal for services related to the COE Program must be submitted within 180 days after you receive
notice of the denial to Premera, not to Regence or Virginia Mason Medical Center. Appeals can be
submitted to:
Premera Blue Cross
Attn: Member Appeals
PO Box 91102
Seattle, WA 98111-9202
Secure inbound fax: 1-425-918-5592
Knee arthroplasty, total
Covered services are paid at the standard rate. Computer navigated and unicompartmental knee
arthroplasty for treatment of end-stage osteoarthritis and rheumatoid arthritis of the knee are covered
only as follows:
• Total knee arthroplasty performed with computer navigation is covered.
2024 UMP CDHP (PEBB) Certificate of Coverage 61
• For individuals with unicompartmental disease, unicompartmental partial knee arthroplasty is covered.
• Multi-compartmental partial knee arthroplasty (including bicompartmental and bi-unicompartmental)
is not covered.
TIP: You may be eligible to have your joint replacement surgery covered in full. See the “Joint
replacement surgery, knees and hips in the Centers of Excellence (COE) Program” benefit.
Mammogram and Digital Breast Tomosynthesis (DBT)
ALERT! Not all mammograms are paid at 100 percent (preventive rate). Only screening
mammograms are considered preventive. Diagnostic mammograms are subject to your
deductible and coinsurance. Claims are paid based on how your provider bills the service.
Screening (preventive)
• For members age 40 or older, with or without a clinical breast exam, the plan covers screening
mammograms and Digital Breast Tomosynthesis (DBT) every year, and they are not subject to your
deductible.
• For members under age 40, the plan covers screening mammograms and DBT for members who are
at an increased risk for breast cancer. A covered health care provider must order the service, and the
claim must be billed with an “at risk” diagnosis to be covered under the preventive care benefit.
Note: Digital Breast Tomosynthesis (DBT) is only covered when you receive it along with a screening
mammogram.
How much you will pay
For all members, services are covered at the preventive rate.
Diagnostic (medical)
You pay the standard rate for medically necessary mammograms to diagnose a medical condition under
the “Diagnostic tests, laboratory, and x-rays” benefit. There are no age requirements for diagnostic
mammograms and DBT. A covered health care provider must order the service, and the claim must be
billed as a diagnostic mammogram.
ALERT! See the “Breast health screening tests” benefit for coverage of diagnostic testing other
than mammograms.
Massage therapy
The plan covers up to 24 visits per calendar year for massage therapy (no more than 90 minutes per visit).
See the definition of “Limited Benefit”. You pay the special rate (a $15 copay) for up to 24 massage
therapy visits per calendar year for covered diagnoses when you see a preferred provider after your
deductible is met. The copay will apply toward the out-of-pocket limit. All visits will apply to the 24-visit
limit. You must have a prescription for massage therapy treatment from a covered provider type, such as a
62 2024 UMP CDHP (PEBB) Certificate of Coverage
physician. The plan does not cover massage therapy when you see a participating or out-of-network
provider.
ALERT! The plan only covers preferred massage therapists. To find a preferred massage
therapist, use the UMP Provider search or contact UMP Customer Service (see Directory for link
and contact information).
Mastectomy and breast reconstruction
ALERT! See page 52 for coverage of breast reconstruction or mastectomy services related to
gender affirming care.
You pay the standard rate for a mastectomy as treatment for disease, illness, or injury, as well as:
• Physical complications of all stages of a mastectomy.
• Prostheses.
• Reconstruction of the breast on which the mastectomy was performed.
• Surgery and reconstruction of the other breast to produce a symmetrical appearance.
Mental health
See the “Behavioral health” benefit.
Naturopathic physician services
While naturopaths are a covered provider type, naturopaths may recommend services that the plan does
not cover. You will pay all costs for excluded and non-medically necessary services, even if your
naturopathic physician recommends or prescribes them (see the “Medically necessary or medical
necessity” definition for more information).
The plan does not cover herbal, homeopathic, or other dietary supplements (including vitamins and
minerals, except as described on page 91), even if a covered provider type prescribes them.
Nurse line
UMP members have access to Advice24 Nurse Triage. Registered nurses are available by phone 24 hours a
day, 7 days a week at no cost to you. Registered nurses provide immediate symptom assessment, health
information, and advice. They can help you decide if you need to go to the emergency room, see a doctor
either virtually or in-person, or care for your symptoms at home. UMP members can call the nurse line at
1-877-375-2599 (TRS: 711).
Nutrition counseling and therapy
TIP: See the “Diabetes education” benefit for how these services are covered for members with
diabetes.
2024 UMP CDHP (PEBB) Certificate of Coverage 63
The plan covers up to 12 visits per lifetime for nutrition counseling and therapy services. Similar services
may be covered under other benefits that are not subject to the 12-visit limit, including, but not limited to,
the “Diabetes Control Program,” “Diabetes education,” and the “Diabetes Prevention Program.”
Obstetric and newborn care
Pregnancy program
As an expectant parent, the program helps you manage your health throughout pregnancy and offers
access to a nurse line, pregnancy support, and education 24 hours a day, 7 days a week. It also includes a
smartphone application to help you track milestones, identify symptoms, access education, and get one-
click access to the nurse line. To enroll in the program, call 1-888-569-2229 (TRS: 711) or sign in to your
Regence account (see Directory for link). This program is covered at no cost to you.
Services for obstetric and newborn care
See the “Covered and noncovered provider types” section for providers whose services are covered by the
plan. Covered professional services include:
• Amniocentesis and related genetic counseling and testing during pregnancy.
• Care of complications associated with pregnancy, including pregnancies resulting from fertility or
infertility treatment.
• Prenatal and postnatal care.
• Prenatal testing (as stated in Washington Administrative Code [WAC] 246-680-020).
• Vaginal or cesarean delivery.
• Placement of IUD including immediately after delivery.
Note: Early elective deliveries may not be covered. See “Deliveries before 39 weeks gestation” below.
For inpatient hospital charges related to a childbirth, you:
• Meet your deductible.
• Pay the coinsurance for professional services while hospitalized.
• Meet your deductible for the newborn. However, if only covered preventive care services (see page 65)
are billed for the newborn, you will not meet your newborn’s deductible or pay the coinsurance when
you see a preferred provider.
Circumcision of the penis is covered as a medical benefit (subject to your deductible and coinsurance).
Because this is not a preventive service, your out-of-pocket cost may include your newborn’s deductible
and coinsurance for professional provider services.
Note: The Newborns’ and Mother’s Health Protection Act (NMHPA) requires a hospital length of stay in
connection with childbirth for a mother or her newborn and may not restrict benefits for the stay to less
than 48 hours following a vaginal delivery or 96 hours following a delivery by cesarean section.
A newborn dependent of a covered gestational parent is covered by the plan from birth to at least 21
days following birth. Even if the newborn is later enrolled in different coverage, the newborn will still be
covered under the gestational parent’s plan coverage for the first 21 days. Visit the HCA website at
hca.wa.gov/erb for what you need to do for continued coverage.
If your obstetric care began while covered under another health plan, and your providers are not part of
the UMP network, contact UMP Customer Service to discuss your options.
64 2024 UMP CDHP (PEBB) Certificate of Coverage
Deliveries before 39 weeks gestation
Vaginal or cesarean deliveries before 39 weeks of gestation are covered when the services are medically
necessary. Examples include:
• A medical emergency affecting the member or baby.
• A medical condition of the member or baby for which a delivery is medically necessary.
• Labor begins naturally (without medical intervention) before the member reaches 39 weeks of
gestation.
Vaginal or cesarean deliveries before 39 weeks of gestation are not covered when the services are:
• Scheduled for convenience and not for medical necessity or medical emergency affecting the member
or baby.
• Neither the member nor baby have a medical condition for which immediate delivery is medically
necessary.
Talk to your provider about whether early delivery is for a medically necessary reason. For questions about
this policy, contact UMP Customer Service.
Services covered as preventive
The following services are covered as preventive (not subject to your deductible or coinsurance when you
see a preferred provider):
• HIV counseling and testing.
• Purchase of manual and electric breast pumps for pregnant and nursing members, plus supplies
included with the initial purchase. Hospital-grade pumps are not covered.
• Screening for diabetes during pregnancy.
See “The UMP Preferred Drug List” section for prescription drugs that are preventive. They are listed as
“Preventive” in the Tier column.
Lactation (breastfeeding) counseling
Lactation counseling is covered at the preventive rate during pregnancy and after birth to support
breastfeeding when members receive services by a covered provider type.
Note: Donor human milk from an approved milk bank for inpatient use may be covered when medically
necessary.
Ultrasounds during pregnancy
The following limits do not apply to high-risk pregnancies. For example, a multiple pregnancy is
considered high risk. Contact UMP Customer Service to learn what is covered for high-risk pregnancies.
Routine ultrasounds during pregnancy are covered as follows:
• One in week 13 or earlier
• One during weeks 13-28
Adding a new dependent to your coverage
For information about how to enroll new dependents in your health plan, refer to the Employee
Enrollment Guide or the Retiree Enrollment Guide on the HCA website at hca.wa.gov/employee-retiree-
benefits/forms-and-publications. You can also refer to “Making changes” in the “Eligibility and
Enrollment” and in the “Eligibility and enrollment for a retiree or survivor” sections of this certificate of
coverage for more information.

2024 UMP CDHP (PEBB) Certificate of Coverage 65
Office visits
The plan pays for office visits for covered conditions under the medical benefit. Preventive care visits with
preferred providers as described under the definition of “Preventive care” are covered in full and are not
subject to your deductible.
Orthognathic and Telegnathic surgery
Orthognathic and telegnathic surgery must be preauthorized by the plan. Contact UMP Customer Service
if you have questions. See page 74 for treatment of temporomandibular joint (TMJ) disorder.
Pain and joint management, interventional
Interventional pain management is a medical subspecialty that treats pain with invasive interventions like
injections, spinal cord stimulations, and implantable drug delivery systems. The purpose of interventional
pain management is to help members have less pain, so they can return to normal activities, when
possible.
Preauthorization is required for interventional pain and joint management, such as:
• Epidural injections
• Facet blocks
• Pain pumps
• Radiofrequency ablations
• Sacroiliac joint injections
Preauthorization is not required for post-procedural pain management in an inpatient setting, including,
but not limited to, treating acute pain due to trauma, acute post-thoracotomy pain, and acute
postoperative pain.
Prescription drugs
See the “Your prescription drug benefit” section.
Preventive care
ALERT! This benefit covers only services that meet the requirements below. If you receive
services during a preventive care visit that do not meet these requirements, or your provider
bills your visit as medical treatment instead of a preventive service, the services are not covered
as preventive. Instead, when medically necessary, they are covered under the standard rate.
Covered preventive care services are paid at the preventive rate. You do not have to meet your deductible
before the plan pays the allowed amount for services covered under the preventive care benefit. When
you see a preferred or participating provider for these services, you pay $0. If you see an out-of-network
provider, you pay 40 percent of the allowed amount, and the provider may balance bill you. If you do not
have access to a preferred or participating provider for preventive care services, see the “When you do not
have access to a preferred provider: network waiver” section for how to request a network waiver.
For a list of services covered as preventive, visit the HealthCare.gov website at healthcare.gov/preventive-
care-benefits. This site also features links to specific preventive services covered for members based on
age and other risk factors. The plan may not cover recommendations added during the calendar year as
preventive until later years. For a list of immunizations covered as preventive, see the “Covered
immunizations” section below.
Examples of services covered under the preventive care benefit include:
• Certain radiology and lab tests, such as screening mammograms (see page 44).

66 2024 UMP CDHP (PEBB) Certificate of Coverage
• Certain screening tests performed during pregnancy (see page 64 for more on prenatal care).
• Fluoride for prevention of dental decay when prescribed by a primary care provider to children ages 17
and under, and when the water source is fluoride deficient (see page 45 for coverage of fluoride
varnish).
• Hearing tests as part of a newborn screening.
• Immunizations as specified under “Covered immunizations” on page 67.
• Intensive behavioral counseling for adults who are overweight or obese and have additional
cardiovascular disease risk factors.
• Certain statin prescription drugs to adults age 40 or older (statin prescription drugs that are listed as
“Preventive” in the Tier column on the UMP Preferred Drug List [see “The UMP Preferred Drug List”
section]).
• One-time screening by ultrasound for abdominal aortic aneurysm for men ages 65-75 who have ever
smoked.
• Preventive vision acuity screening from birth through 18 years of age.
• Preventive visits such as well-baby care and annual physical exams.
• Routine screenings for adults.
• Screening for hepatitis B for adolescents and adults at high risk and those who are pregnant.
• Screening procedures, such as colonoscopy (see page 48 for coverage of colonoscopy performed to
diagnose or treat disease or illness). If you have a screening and the provider diagnoses and treats a
condition during the colonoscopy, services will be paid at the standard rate.
Note: Prostate cancer screening (prostate-specific antigen [PSA testing]) is not covered under the
preventive care benefit but is covered as a medical benefit (subject to your deductible and coinsurance).
For more information, see page 48.
ALERT! Follow-up visits or tests as a result of your preventive care visit are not covered under
the preventive care benefit. If the plan normally covers the test or visit and it is medically
necessary, it is covered under the medical benefit.
Contact UMP Customer Service to ask if a medical service is covered as preventive. Contact WSRxS
Customer Service for questions about preventive prescription drugs.
The following specific services are covered as preventive:
• Chlamydia and gonorrhea testing in sexually active women ages 24 and younger, and for women age
25 or older who are at increased risk for infection.
• Counseling and screening for HIV, counseling and screening for interpersonal and domestic violence,
and counseling for sexually transmitted infections.
• Education and counseling regarding contraception.
• Human Papillomavirus (HPV) testing for women age 30 or older, once every three years.
For additional services covered as preventive, see the following benefits: “Family planning services,”
“Mammogram and Digital Breast Tomosynthesis (DBT),” and “Obstetric and newborn care.”

2024 UMP CDHP (PEBB) Certificate of Coverage 67
Preventive care for specified chronic conditions
UMP covers services and supplies when prescribed to prevent the worsening of a diagnosed chronic
condition or the development of a secondary condition. You pay coinsurance, but these services or
supplies are not subject to any applicable deductible when received from a preferred or participating
provider.
Prescription drug benefit
• Certain medications covered through the prescription drug benefit as outlined on the UMP Preferred
Drug List;
• Continuous glucose monitors (purchase at a network pharmacy to avoid balance billing); or
• Glucometers (purchase at a network pharmacy to avoid balance billing).
Medical benefit
• Blood pressure monitor if you have a diagnosis of high blood pressure;
• Hemoglobin A1c testing, and retinopathy screening if you have a diagnosis of diabetes;
• International Normalized Ratio (INR) testing if you have a diagnosis of liver disease and/or bleeding
disorders;
• Low-Density Lipoprotein (LDL) testing if you have a diagnosis of heart disease; or
• Peak flow meter if you have a diagnosis of asthma.
Covered immunizations
You pay the standard rate for covered immunizations that are not considered preventive.
The plan covers immunizations listed on the Centers for Disease Control and Prevention (CDC) applicable
immunization schedule (children, adolescents, adults) for U.S. residents. For a list of immunizations
covered as preventive, visit the CDC website at cdc.gov/vaccines/schedules/index.html or contact UMP
Customer Service.
Some covered immunizations are classified as “may be recommended” by the CDC depending on medical
condition or lifestyle. For those immunizations to be covered as preventive, you must meet the criteria
specified on the CDC schedule.
Immunizations covered under the preventive rate are not subject to your deductible. Covered
immunizations given by the providers listed under the “Where to get immunizations” section below are
paid under the preventive care benefit. If you see an out-of-network provider for covered preventive
immunizations, you pay 40 percent of the allowed amount and the provider may balance bill you. Flu
shots and COVID-19 vaccines are paid at 100 percent regardless of the provider’s network status.
TIP: The plan covers flu shots and COVID-19 vaccines listed on the applicable CDC
immunization schedule. For a list of immunizations covered as preventive, find a link to the
CDC immunization schedules at the CDC website at cdc.gov/vaccines/schedules/index.html or
contact UMP Customer Service.
Where to get immunizations
You pay $0 for immunizations covered under the preventive care benefit when received from a:
• Preferred or participating provider.
68 2024 UMP CDHP (PEBB) Certificate of Coverage
• Network vaccination pharmacy (Many network pharmacies have vaccination pharmacists who may give
covered preventive immunizations to members. Contact a network pharmacy ahead of time to make
sure the pharmacy has the vaccine you need. Present your UMP member ID card at the pharmacy
counter for billing before receiving a vaccine.)
• Public health department.
The plan does not cover immunizations for travel or employment, even when recommended by the CDC
or required by travel regulations. Exception: COVID-19 vaccines are covered when required for
employment.
TIP: If you get a vaccine from an out-of-network provider, submit your claim to Regence
BlueShield as a medical claim (see the “Billing and payment: submitting a claim” section). If you
get a vaccine from an out-of-network pharmacy, submit your prescription drug claim to WSRxS
(see the "Submitting a claim for prescription drugs" section). If you use an out-of-network
provider or an out-of-network pharmacy, services will be paid at the out-of-network rate and
you may be balance billed. Vaccines from an excluded pharmacy will not be covered. See the
definition of “Excluded pharmacy.”
Radiology
Preauthorization is required for all non-emergency diagnostic imaging. Providers should obtain
preauthorization before scheduling or performing any elective outpatient imaging service. Examples of
imaging tests that require a preauthorization are:
• Computed tomography (CT)
• Computed tomography angiography (CTA)
• Magnetic resonance angiography (MRA)
• Magnetic resonance imaging (MRI)
• Myocardial perfusion imaging (MPI)
• Nuclear cardiology:
▪ Blood pool imaging
▪ First pass ventriculography
▪ Infarct imaging
▪ Multiple-gated acquisition (MUGA) scan
• Positron emission tomography (PET and PET-CT)
Second opinions
This benefit covers:
• Second opinions you choose to get. The plan covers these under the medical benefit, once you meet
your deductible and pay the coinsurance.
• Second opinions required by the plan. The plan covers these at 100 percent (you do not have to
meet your deductible or pay the coinsurance). If you do not get a second opinion when required by the
plan, coverage for services may be denied.
2024 UMP CDHP (PEBB) Certificate of Coverage 69
• Expert Second Opinion program. This program, provided by 2nd.MD, offers members the
opportunity to consult virtually with specialists. It also provides for expert lead consultation and post-
consultation follow-up support. To learn more visit the 2nd.MD website at 2nd.md/ump or call 1-866-
982-1434 (TRS: 711).
Skilled nursing facility
Skilled nursing facility services are paid at the inpatient rate. The plan must preauthorize services before
you are admitted to a skilled nursing facility (see the “Limits on plan coverage” section). In addition, the
facility must notify the plan within 24 hours of your admission (see page 104).
This benefit covers skilled nursing facility charges for services, supplies, and room and board, including
charges for services such as general nursing care made in connection with room occupancy. The plan
covers up to 150 days per calendar year. Room and board is limited to the skilled nursing facility’s average
semiprivate room rate, except where a private room is determined to be medically necessary.
The plan does not cover stays at a skilled nursing facility that are primarily convalescent or custodial in
nature.
Private duty nursing furnished by a licensed home health agency may be substituted as an alternative to
placement at a skilled nursing facility only if:
• Skilled nursing facility care is medically necessary, not primarily convalescent or custodial in nature, and
would be covered by the plan;
• Private duty nursing is the most cost-effective setting (private duty nursing must be an equal or lesser
cost compared to a nursing facility); and
• The member's provider agrees that private duty nursing is medically appropriate and will adequately
meet the member's needs.
Private duty nursing is shift-based, hourly nursing care at home for adults and children, typically with a
chronic illness, injury, or disability.
Substitution of private duty nursing in lieu of placement in a skilled nursing facility has the same
requirements and limitations as the facility benefit. For example, all deductibles and coinsurances apply
and the benefit is limited to the equivalent of a maximum of 150 skilled nursing facility days per calendar
year.
Sleep therapy
Preauthorization is required for any facility-based diagnostic or titration study (free-standing or hospital),
and for sleep treatment equipment and related supplies, such as:
• Initial treatment order and supplies (APAP, CPAP, BiPAP).
• In-lab sleep study (PSG, MSLT, MWT).
• Ongoing Treatment Order (APAP, CPAP, BiPAP).
• Titration study.
Exception
The following supplies do not require a preauthorization:
• Ongoing APAP supplies
• Ongoing BiPAP supplies
• Ongoing CPAP supplies
70 2024 UMP CDHP (PEBB) Certificate of Coverage
Locations where sleep therapy services are not covered
Sleep therapy services are not covered:
• In the emergency room
• At urgent-care facilities
• During inpatient hospitalization
Spinal and extremity manipulations
The plan covers up to 24 visits per calendar year for manipulations (adjustments) of the spine and
extremities (arms and legs). See the definition of “Limited benefit.”
You pay the special rate (a $15 copay) for up to 24 visits for spinal and extremity manipulations when you
see a preferred provider after you meet your deductible. The copay will apply toward the out-of-pocket
limit. All visits apply to the 24-visit limit.
You may receive an office visit (see the “Office visits” benefit for more details) and/or x-ray (see the
“Diagnostic tests, laboratory, and x-rays” benefit for more details) at the time of your spinal and extremity
manipulation service.
Note: For participating providers and out-of-network providers, services are paid at the standard rate up
to 24 visits per calendar year.
Spinal injections
The plan must preauthorize some spinal injections (see the “Limits on plan coverage” section for how this
works). The following therapeutic injections are covered for treatment of chronic pain:
• Cervical-thoracic epidural injections
• Lumbar epidural injections
• Sacroiliac joint injections
Note: See page 114 for a list of spinal injections that are not covered by the plan.
Spinal injections not specified in this section may be covered subject to the plan’s medical policy. Contact
UMP Customer Service for more information.
Spinal surgery
The plan must preauthorize inpatient and outpatient spinal surgery performed outside of the Centers of
Excellence (COE) Program.
Spine care in the Centers of Excellence (COE) Program
The Centers of Excellence (COE) Program covers 100 percent of the allowed amount for covered services
after you meet your deductible related to lumbar fusion. The program includes, but is not limited to:
• An evaluation to determine if surgery is appropriate.
• Presurgical consultations.
• Travel costs (see the “Travel benefits” section below).
• Hospitalization and surgery, if surgery is determined to be appropriate.
• Postsurgical check-ups.
In the COE program, members work with Premera Blue Cross (the administrator of the program) and
Virginia Mason Medical Center (the Center of Excellence) to make sure that their treatment is consistent
with established standards of medical care.
2024 UMP CDHP (PEBB) Certificate of Coverage 71
Premera will help you understand how the COE Program works, what is covered under the Program,
connect you with Virginia Mason Medical Center providers if you are eligible, and work to resolve any
questions or issues you may have.
If you receive services related to spine care that are not covered under the COE Program, but are covered
under the plan, you will pay your normal UMP cost-share, depending on the services received and the
network status of the provider(s). This may be a deductible, coinsurance, or amounts not covered by the
plan. Services billed to the plan outside of the COE Program are subject to the plan’s preauthorization
requirements.
Center of Excellence for spine care: Virginia Mason Medical Center
Virginia Mason Medical Center is the provider approved to perform spine care evaluations and surgeries
under the COE Program. This facility has proven that they provide high-quality spine care using the most
up-to-date medical guidelines and services.
Who is eligible to participate in the COE Program?
You are eligible to participate in the COE Program if you are:
• A member enrolled in UMP CDHP.
• Not enrolled in Medicare as your primary coverage.
• Age 18 or older.
How to apply to participate in the COE Program
If you are interested in participating in the COE Program:
• You may self-refer by calling Premera at 1-855-784-4563 (TRS: 711).
• Your regular provider may refer you.
You may receive information in the mail about the COE Program, which will explain how the program
works and whom to contact for more information. Premera will screen applicants to initially determine
whether they are eligible to participate in the COE Program.
What happens after you are approved to participate
After you are approved to participate in the program, Premera will:
• Provide a booklet to participants describing their journey through the program.
• Assign participants a dedicated case manager who will walk participants through each step of the
journey.
• Gather relevant medical records to supply to the participant’s COE care team as part of the referral
process. This information helps the care team assess next steps
After Premera’s referral, Virginia Mason Medical Center will review participant’s medical records and
schedule an evaluation appointment to determine whether the surgery is medically appropriate for the
participant under the COE Program.
Virginia Mason Medical Center must determine if surgery for spine care is appropriate based on
established medical guidelines. You may find these guidelines on the Policies that affect your care
webpage (see Directory for link).
What is included in the COE Program
In general, all eligible expenses associated with a spine care evaluation and a spine care surgery (if
determined surgically appropriate) under the COE Program are covered. If surgery is recommended, this
includes expenses from the day you arrive for your pre-operative visit through discharge, including your:

72 2024 UMP CDHP (PEBB) Certificate of Coverage
• Assessment(s).
• Surgery.
• Hospital stay.
• Hospital discharge (excluding take-home prescription drugs, which are covered under your UMP
prescription drug benefit).
Travel benefits
Members participating in the COE Program may qualify for assistance with travel and lodging expenses.
These expenses may include partial coverage by Premera for mileage, flights, parking, and lodging.
To be covered by the program, all travel must be arranged through Premera. This travel may be
arranged by calling Premera at 1-855-784-4563 (TRS: 711).
You must have an approved adult care companion, whose travel expenses will be covered as described
below. You may be partially reimbursed for expenses related to:
• Mileage for driving within Washington. To qualify for reimbursement for mileage, members must live at
least 60 driving miles from Virginia Mason Medical Center, located at 1100 9th Ave., Seattle, WA 98101.
• Flights departing from and arriving at airports within Washington or Portland International Airport. You
must depart from the airport closest to your residence.
• Ground transportation from Seattle-Tacoma International Airport to Virginia Mason Medical Center.
• Lodging expenses (excluding meals) at a COE-designated hotel. Premera must arrange all lodging.
• Parking at Virginia Mason Medical Center and parking at your departing airport.
TIP: Reimbursement for travel expenses is based on cost or current IRS rates for medical
expenses, whichever is less, and may not cover all of your costs. For the IRS rates, visit the IRS
website at irs.gov/tax-professionals/standard-mileage-rates.
What is not included in the COE Program
If you receive spine care services outside of the COE Program, or choose to receive services at Virginia
Mason Medical Center that are not related to your spine care evaluation or surgery, covered services will
be processed at the standard rate.
The following services are not included in the COE Program (but may be covered by other plan benefits):
• Care received as part of the plan Virginia Mason Medical Center gives you as a condition of surgery,
regardless of where you receive care. Examples include tobacco cessation and weight loss programs.
• Physical therapy that is not provided during your hospitalization.
• Follow-up care other than the initial postsurgical checkup at Virginia Mason Medical Center. An
example of follow-up care is a visit with your regular doctor.
• Prescription drugs received from a pharmacy after discharge from the hospital.
• Convenience items, such as a personal phone.
Contact UMP Customer Service if you have questions about services not included in the COE Program.
2024 UMP CDHP (PEBB) Certificate of Coverage 73
What happens if you are not an appropriate candidate for spine care surgery
under the COC Program
If Virginia Mason Medical Center determines you are not an appropriate candidate for spine care surgery,
you may still receive spine care surgery through other providers under this plan. Services received outside
the COE Program are processed according to the plan’s medical policies, benefit structure, and the
network status of your provider.
Appeals related to the COE Program
UMP members may appeal denials made by Premera. Appeals must be submitted to Premera. A decision
by your Virginia Mason Medical Center provider regarding whether the provider is willing to perform
spine care surgery on you is a decision of the provider, not the plan, and cannot be appealed to the plan
or Premera.
TIP: Appeal deadlines and other rules remain the same. See the “Complaint and appeal
procedures” section for details of how non-COE appeals work.
An appeal for services related to the COE Program must be submitted within 180 days after you receive
notice of the denial to Premera, not to Regence or Virginia Mason Medical Center. Appeals can be
submitted to:
Premera Blue Cross
Attn: Member Appeals
PO Box 91102
Seattle, WA 98111-9202
Secure inbound fax: 1-425-918-5592
Substance use disorder
See the “Behavioral health” benefit.
Surgery
Note: When you receive nonemergency services at a network hospital, network hospital
outpatient department, network critical access hospital, or network ambulatory surgical center
in Washington State, you pay the network rate and cannot be balance billed regardless of the
network status of the provider. For nonemergency services performed at one of these facilities
outside of Washington State, you still pay the network rate, but in some states, an out-of-
network provider may be allowed to ask you to waive some of your balance billing protections.
You pay the standard rate for covered surgical services. The plan pays for covered surgical services
according to the network status of the provider. The surgeon and other professional providers may bill
separately from the facility.
Your provider must notify the plan when you are admitted for inpatient treatment and when you receive
certain services. Some outpatient procedures require preauthorization. Find the list of services that require
preauthorization on the UMP Policies that affect your care webpage. Contact UMP Customer Service if
you have questions. See Directory for link and contact information.

74 2024 UMP CDHP (PEBB) Certificate of Coverage
The plan covers the following services as outpatient:
• Outpatient surgery at a hospital
• Short-stay obstetric (childbirth) services (released within 24 hours of admission)
• Surgery and procedures performed at an ambulatory surgery center
ALERT! All surgeries must follow the plan’s coverage rules. We recommend that you contact
UMP Customer Service before any procedure to ask if it is covered or requires
preauthorization.
Temporomandibular joint (TMJ) disorder treatment
The plan covers diagnosis and medically necessary treatment of temporomandibular joint (TMJ) disorders,
including surgery and non-surgical services. Treatment must follow the plan’s medical policy and requires
preauthorization. Treatment that is experimental or investigational, or primarily for cosmetic purposes, is
not covered.
Therapy: Habilitative and Rehabilitative
Note: The total limit for therapies for inpatient habilitative and inpatient rehabilitative services is a
combined limit of 60 days annually. The total limit for therapies for outpatient habilitative and outpatient
rehabilitative services is a combined limit of 60 visits annually.
Habilitative (Neurodevelopmental) Services
The plan covers inpatient and outpatient habilitative (neurodevelopmental) services to assist a person to
keep, learn, or improve skills and functioning for daily living. This could be related to issues such as:
• A congenital anomaly (such as cleft lip or palate).
• Conditions of developmental delay, including autism.
For the purposes of this benefit, developmental delay means a significant lag in achieving skills such as:
• Cognitive (thinking).
• Language (speech, reading, writing).
• Motor (crawling, walking, feeding oneself).
• Social (getting along with others).
You must have a prescription for occupational, physical, and speech therapy services from a covered
provider type (see the “Covered and noncovered provider types” section), such as a physician.
Inpatient habilitative services
Preauthorization is required for inpatient habilitative admissions. The plan covers therapy services when
they are provided during inpatient habilitative admission, up to 60 days combined per calendar year,
counting all types of therapies listed here (see definition of “Limited benefit”). You must pay your
coinsurance for inpatient services.
Outpatient habilitative services
The plan covers medically necessary outpatient occupational, physical, and speech therapy services up to
60 visits combined per calendar year, counting all types of therapies listed here (see definition of “Limited
benefit”).
2024 UMP CDHP (PEBB) Certificate of Coverage 75
Rehabilitative Services
The plan covers inpatient and outpatient services to improve or restore function lost due to issues such as:
• An illness.
• An acute injury.
• Worsening or aggravation of a chronic injury.
You must have a prescription for occupational, physical, and speech therapy services from a covered
provider type (see the “Covered and noncovered provider types” section, such as a physician.
Inpatient rehabilitation services
Preauthorization is required for inpatient rehabilitation admissions. The plan covers therapy services when
they are provided during inpatient rehabilitation admission, up to 60 days combined per calendar year,
counting all types of therapies listed here (see definition of “Limited benefit”). You must pay your
coinsurance for inpatient services.
Outpatient rehabilitation services
The plan covers medically necessary outpatient neurodevelopmental, occupational, physical, and speech
therapy services up to 60 visits combined per calendar year, counting all types of therapies listed here (see
definition of “Limited benefit”).
Tobacco cessation services
ALERT! If you get nicotine replacement therapy or prescription drugs for tobacco cessation at
a non-network pharmacy, or purchase at a cash register other than the pharmacy counter, and
submit a claim, you may not receive full reimbursement from the plan. See the “Where to buy
your prescription drugs” section for how to locate a network pharmacy. Prescriptions
purchased from an excluded pharmacy will not be covered. See the definition of “Excluded
pharmacy.”
The services described in this section are covered only for tobacco cessation. Nicotine replacement
therapy and prescription drugs for tobacco cessation that are listed as “Preventive” in the Tier column on
the UMP Preferred Drug List are not subject to your deductible or coinsurance.
If you purchase an over-the-counter tobacco cessation product without a valid prescription, the plan will
not cover it and you will pay the full cost.
TIP: You do not have to enroll in the tobacco cessation program to get coverage of nicotine
replacement therapy or prescription drugs for tobacco cessation. See below for limits and rules
on accessing these services.
Nicotine replacement therapy
The plan covers only certain nicotine replacement therapy products (such as gum, patches, sprays,
inhalers, tablets, or lozenges) at the preventive rate. Those that are preventive are listed as “Preventive” in
the Tier column on the UMP Preferred Drug List. The plan does not normally cover over-the-counter
drugs, but the plan covers nicotine replacement products when they are purchased at a network
pharmacy using your UMP member ID card.

76 2024 UMP CDHP (PEBB) Certificate of Coverage
You may get nicotine replacement therapy directly from the tobacco cessation program (see the “Tobacco
cessation program” section below), or by following these steps:
1. Get a prescription from your provider.
2. Take the prescription to a network pharmacy.
3. Make your purchase at the pharmacy counter of a network pharmacy. Give your prescription and
your UMP member ID card to the pharmacist. The purchase must be submitted through the
prescription drug system to be covered. If you do not provide a valid prescription at the pharmacy
counter, the plan will not cover it.
If you get a nicotine replacement therapy product not designated as preventive, the plan will not cover it,
and you will pay the full cost. To request full coverage of non-preventive nicotine replacement therapy for
a medical reason, see “How to request an exception” below.
The plan does not cover e-cigarettes or vaporizers (“vapes”).
Counseling
The plan covers in-person counseling related to tobacco cessation at the preventive rate when you see a
preferred or participating provider.
Phone or online counseling is covered only through the Tobacco cessation program described below.
UMP members ages 17 and under may use the Smokefree Teen program as explained below.
How to request an exception
To request coverage of a prescription drug or nicotine replacement therapy not usually covered under this
benefit, see “Requesting an exception for noncovered prescription drugs” on page 89 for how to request
an exception. If your exception is approved, you will receive the approved product or prescription drug at
no cost.
Tobacco cessation program
UMP members age 18 or older may participate in the tobacco cessation program. The program offers a
variety of resources, including phone counseling, medications, personalized coaching, web tools,
educational materials, nicotine replacement therapy, and other resources to help you stop tobacco use. It
also offers a free personalized quit plan and has been proven to help individuals quit more successfully
than trying to quit without support. To learn more, visit the UMP Care programs webpage at
ump.regence.com/pebb/benefits/programs.
If you get nicotine replacement therapy or prescription drugs for tobacco cessation that are not listed as
“Preventive” in the Tier column on the UMP Preferred Drug List, you will pay as described in the “Nicotine
replacement therapy” section on page 75.
For nicotine replacement therapy, you may get supplies sent to you from the program or get a
prescription from your provider and purchase as described under “Nicotine replacement therapy” on page
75.
ALERT! You may attest for an exemption to the PEBB tobacco use premium surcharge if you or
a dependent are tobacco-free for two months, enroll in the tobacco cessation program (for
members age 18 or older), or access the information and resources aimed at teens in
Smokefree Teen (for members ages 13 through 17). Visit the HCA website at hca.wa.gov/erb
for details about the surcharge.
2024 UMP CDHP (PEBB) Certificate of Coverage 77
Smokefree Teen
UMP members ages 17 and under may access tobacco cessation support services through the Smokefree
Teen program online at teen.smokefree.gov or by calling 1-800-QUIT-NOW (784-8669) (TRS: 711).
Transplants
You must receive preauthorization from the plan for all transplants (except kidney and cornea). This
benefit covers services related to transplants, including professional and facility fees for inpatient
accommodation, diagnostic tests and exams, surgery, and follow-up care.
Donor coverage
If a UMP member receives an organ, eye, or tissue donation from a live donor, the plan pays the standard
rate for the donor’s covered expenses as primary, regardless of any other coverage the donor may have.
Covered donor expenses include costs to remove the donor’s organ and treat complications directly
resulting from the donor’s surgery.
Urgent care
See the “Emergency room” benefit for care during a medical emergency.
If you need immediate care or need care when your usual provider is closed, and your situation is not a
medical emergency, you may use urgent care facilities to receive care at a lower cost than an emergency
room. These services are paid at the standard rate, according to the provider’s network status. Visit the
UMP Provider search to find preferred urgent care facilities (see Directory for link).
Virtual care
Telemedicine services
Telemedicine is the delivery of health care services through audio and visual technology, allowing real-
time communication between the member at the originating site and a provider for the purpose of
diagnosis, consultation, or treatment. Telemedicine includes audio-only telemedicine. Telemedicine does
not include the use of fax or email.
“Store and forward technology” is a term used for the transfer of a member’s medical information from
one health care provider to another at a distant site, which results in medical diagnosis and management
of the covered person. The purpose of telemedicine and store and forward technology is diagnosis,
consultation, or treatment of the member. It does not include the use of fax or email.
If you see a network provider, telemedicine services are paid at the network rate. If you see an out-of-
network provider, telemedicine services are paid at the out-of-network rate.
The plan covers store and forward technology and telemedicine from authorized originating sites under
the medical benefit if:
• The plan provides coverage for the service when provided in person by the provider;
• The service is medically necessary;
• The service is determined to be safely and effectively provided through telemedicine or store and
forward technology according to generally accepted health care practices and standards;
• The technology used to provide the service meets the standards required by state and federal laws
governing the privacy and security of protected health information; and
• The service is recognized as an essential health benefit under section 1302(b) of the federal Patient
Protection and Affordable Care Act (PPACA) in effect on January 1, 2015.
78 2024 UMP CDHP (PEBB) Certificate of Coverage
If services are provided through store and forward technology, there must be an associated office visit
between the covered person and the referring health care provider. The associated office visit may be in
person or via telemedicine. For audio-only telemedicine, the member must have an established
relationship with the provider.
The originating site (the member’s physical location) for telemedicine services must be one of the
following sites:
• Community mental health center
• Federally qualified health center
• Home or any location determined by the
individual receiving the service
• Hospital
• Physician's or other health care provider's
office
• Renal dialysis center (except independent
renal dialysis center)
• Rural health clinic
• Skilled nursing facility
Any originating site, except home, may charge a facility fee for infrastructure and preparation of the
member.
Telemedicine and store and forward technology are subject to all terms and conditions of the plan,
including utilization review, preauthorization requirements, and deductible. Services obtained from out-
of-network providers will be reimbursed at the out-of-network rate.
The following are not covered by the plan:
• Email or fax transmissions between provider and member
• Home health monitoring
• Installation or maintenance of any telecommunication devices or systems
• Originating sites’ professional fees
• Services that are not medically necessary
• Services that would not be covered if delivered in person
• Store and forward technology without an associated office visit between the covered member and the
referring health care provider
• Telemedicine or store and forward services for services that are not recognized as essential health
benefits under section 1302(b) of the PPACA in effect on January 1, 2015
• Telemedicine or store and forward services that cannot be safely and effectively provided through
telemedicine or store and forward technology
• Telemedicine or store and forward services that use technology that does not meet state and federal
requirements for privacy and security of protected health information
• Telemedicine visits originating from a location other than the specified originating sites
Doctor On Demand
Doctor On Demand is a virtual care service that gives you access to providers 24 hours a day, 7 days a
week. It is a good option to consider when you need medical attention, but not emergency room or
urgent care. Doctor On Demand providers are board-certified, U.S.-based providers who are specifically
trained in video medicine. Members can connect in minutes with doctors face-to-face through a
smartphone, tablet, or computer via the website or Doctor On Demand smartphone application. To learn
more, visit the Telemedicine (virtual care) webpage at ump.regence.com/pebb/benefits/telemedicine.
2024 UMP CDHP (PEBB) Certificate of Coverage 79
Providers review a member's history and symptoms, perform an exam, and recommend treatment, which
may include prescription drugs and lab work. Doctor On Demand providers can treat most common
health conditions, including, but not limited to:
• Asthma.
• Colds and allergies.
• Diabetes.
• Eczema and acne.
• Heartburn and indigestion.
• High blood pressure and high cholesterol.
• Migraines.
• Pink eye.
• Urinary Tract Infections (UTIs).
A Doctor On Demand virtual care appointment is paid at the standard rate. Doctor On Demand providers
are considered preferred providers.
Doctor On Demand does not include the use of audio-only telephone, fax, or email. For additional
questions, contact UMP Customer Service.
Vision care (diseases and disorders of the eye)
You pay the standard rate under the medical benefit for treatment of diseases and disorders of the eye
that are not part of a routine vision exam. Orthoptic therapy is not covered except for the diagnosis of
strabismus, a muscle disorder of the eye. LASIK surgery is not covered.
Following cataract surgery, vision hardware (contact lenses or eyeglasses, including frames and
prescription lenses) is covered as DME (see page 48). These services are paid at the standard rate.
Your routine vision benefits
Vision coverage is provided by UMP, in collaboration with Regence Choice Vision Plan administered by
Vision Service Plan (VSP). Regence BlueShield administers benefits for the treatment of diseases and
disorders of the eyes. VSP administers benefits for routine eye exams and hardware (prescription lenses,
frames or prescription contact lenses) and provides claims administration for this plan.
When you have questions about treatment of diseases and disorders of the eyes contact UMP Customer
Service. When you have questions about routine eye exams and hardware, call VSP Member Services at
1-844-299-3041 or TTY 1-800-428-4833.
See the Directory at the beginning of the COC for vision services contact information.
Finding a routine vision provider
Get the most out of your UMP vision benefits and save money with a VSP Choice network provider. As a
UMP member, you may search for a VSP Choice network provider for preventive (routine) vision services
through the VSP website by logging in to your VSP account or by selecting “Find a doctor,“ and using the
advanced search option to select “Choice” for “Doctor network.“ You can also search by signing in to your
Regence account, selecting “Find care,” and selecting “Vision.” See the Directory pages at the beginning of
this booklet for links and contact information. Members under age 19 do not have out-of-network
provider benefits.
• VSP Choice network provider: When you choose to see a VSP Choice network provider for covered
preventive vision care, you pay $0 of the allowed amount and the plan pays 100 percent of the allowed
amount. Select a VSP Choice network provider who participates in the Premier Program to receive the
best value for lenses and frames or contact lenses. VSP providers who participate in the Premier
Program provide access to special offers and savings.
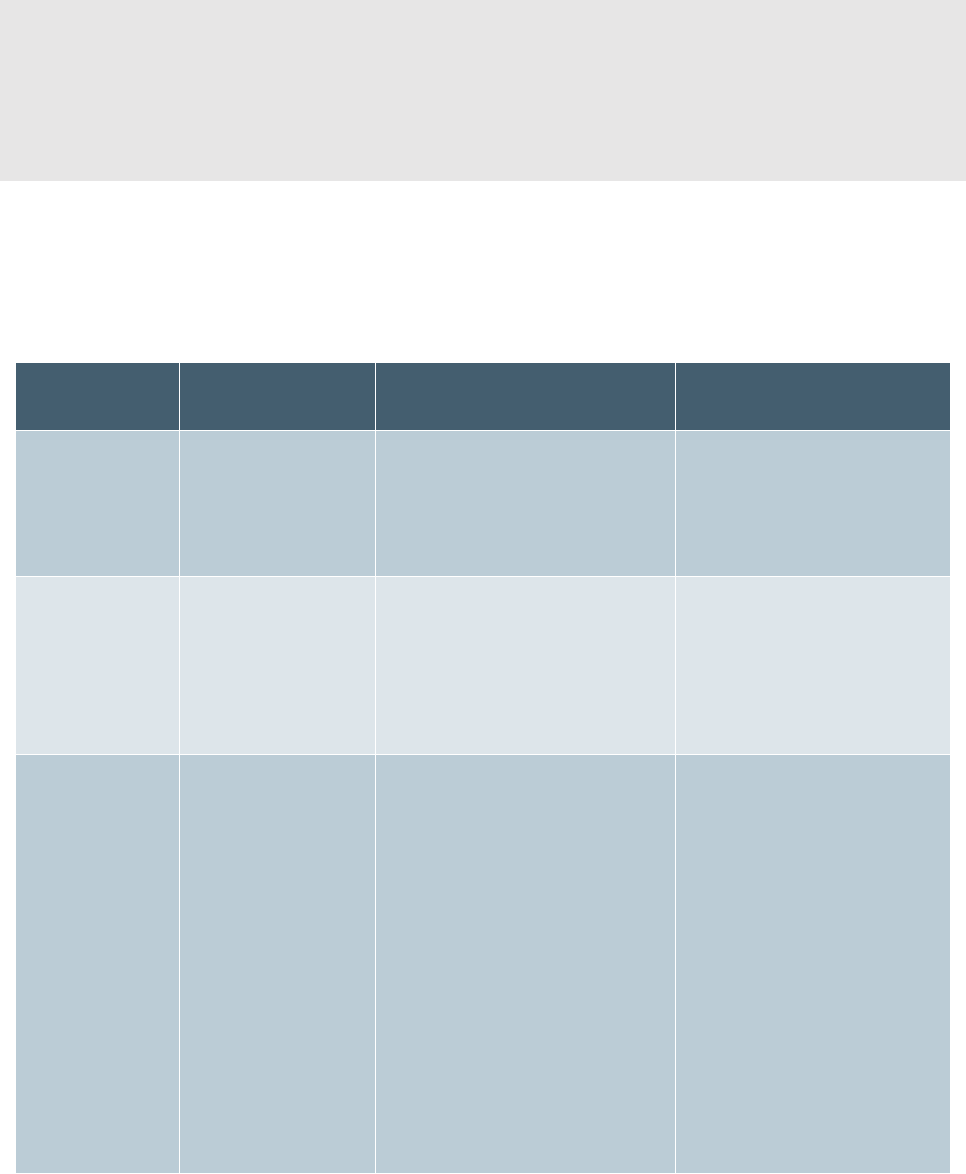
80 2024 UMP CDHP (PEBB) Certificate of Coverage
• Out-of-network provider: For members age 19 or older, out-of-network providers will cost you more.
See the table below for more information. Members under age 19 do not have out-of-network
benefits.
ALERT! This benefit covers only services that meet the requirements below. If you receive
services during a comprehensive routine eye exam and your provider bills your visit as a
medical treatment instead of as a routine service, the services are not covered as routine.
Instead, when medically necessary, they may be covered under your medical benefits. See the
“Vision care (diseases and disorders of the eye)” benefit for more information.
Adults (age 19 or older)
This section explains how the plan pays for covered services for members age 19 or older. The explanation
includes information about maximum benefits, covered services, and payment. The below VSP coverage
table applies to adults and dependents age 19 or older.
Benefit
Frequency
Your cost with a VSP Choice
network provider
Your cost with an out-of-
network provider
Professional
comprehensive
routine eye
exams
One per calendar
year.
You pay $0 of the allowed
amount and the plan pays
100% of the allowed amount.
You pay 100% of billed
charges.
VSP will reimburse you up to
$45 when you submit a
claim for a covered exam.
Frames
One every two
calendar years.
You pay $0 up to a $150 frame
allowance; or
You pay $0 up to an $80 frame
allowance for Walmart®,
Sam’s Club®, or Costco®
providers.
You pay 100% of billed
charges.
VSP will reimburse you up to
$70 when you submit a
claim for covered frames.
Lenses and
enhancements
One set every two
calendar years.
You pay $0 for the following
covered lenses and the plan
pays 100% of the allowed
amount:
• Single vision lenses
• Lined bifocal lenses
• Standard progressive lenses
• Lined trifocal lenses
• Lenticular lenses
Note: Lens enhancement is not
covered except for impact-
resistant coating for dependent
children age 19 or older.
You pay 100% of billed
charges.
VSP will reimburse you up to
the following amounts when
you submit a claim for
covered lenses:
• $30 single vision lenses
• $50 lined bifocal lenses
• $50 standard progressive
lenses
• $65 lined trifocal lenses
• $100 lenticular lenses
2024 UMP CDHP (PEBB) Certificate of Coverage 81
Benefit
Frequency
Your cost with a VSP Choice
network provider
Your cost with an out-of-
network provider
Contacts
One set of contact
lenses or
disposable contact
lenses up to the
maximum
allowance instead
of frames and
lenses every two
calendar years.
You pay $30 copay for a
contact lens evaluation and
fitting exam.
You pay $0 up to a $150
contact allowance for elective
contact lenses.
You pay $0 for necessary
contact lenses. Note: You are
still responsible for paying a
$30 copay for the contact lens
evaluation and fitting exam.
You pay 100% of billed
charges.
VSP will reimburse you up to
the following amounts when
you submit a claim for
contact lenses:
• $105 for elective contact
lenses
• $210 for necessary
contact lenses
Note: See below for reimbursement rates for vision services received outside the U.S.
Vision exam
You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount when you see a
VSP Choice network provider for one professional comprehensive routine eye examination with refraction
or visual analysis per calendar year, including:
• Prescribing and ordering proper lenses;
• Verifying the accuracy of the finished lenses; and
• Progress or follow-up work as necessary.
• When you see an out-of-network provider you pay 100 percent of the billed charges. VSP will
reimburse you up to $45 when you submit a claim for covered services.
• When you receive services outside the country, you pay 100 percent of the billed charges. VSP will
reimburse you up to $80 when you submit a claim for covered services.
Vision hardware
Lenses for glasses
You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount once every two
calendar years for one set of covered glass or plastic lenses:
• Single vision lenses
• Lined bifocal lenses
• Lined trifocal lenses
• Lenticular lenses
• Standard progressive lenses
• Lens enhancement covered for dependent children age 19 or older only:
▪ Impact-resistant coating
When you see an out-of-network provider you pay 100 percent of the billed charges. When you submit a
claim for covered lenses, VSP will reimburse you up to the following amounts:
• $30 single vision lenses
• $50 lined bifocal/standard progressive lenses
82 2024 UMP CDHP (PEBB) Certificate of Coverage
• $65 lined trifocal lenses
• $100 lenticular lenses
When you receive services outside the country, you pay 100 percent of the billed charges. When you
submit a claim for covered lenses, VSP will reimburse you up to the following amounts:
• $70 single vision lenses
• $80 lined bifocal/standard progressive lenses
• $90 lined trifocal lenses
• $125 lenticular lenses
Frames
The plan covers one frame every two calendar years:
• When you see a VSP Choice network provider, the plan pays up to $150. You pay any amount over
$150.
• When you see an out-of-network provider you pay 100 percent of the billed charges. VSP will
reimburse you up to $70 when you submit a claim.
• When you see a VSP approved wholesale/retail vendor the plan pays up to the VSP approved
wholesale/retail limit of $80. You pay any amount over $80. VSP approved wholesale/retail vendors
include both community-based providers, as well as national retail chains. For a list of wholesale/retail
vendors, contact VSP Member Services at 1-844-299-3041 or TTY 1-800-428-4833.
• When you receive services outside the country, you pay 100 percent of the billed charges. When you
submit a claim, VSP will reimburse you up to $150.
Contact lenses
The plan covers elective contact lenses or necessary contact lenses in lieu of frames and lenses once every
two calendar years.
• Elective contact lenses are contact lenses that are covered under the frame limit in lieu of coverage
for eyeglasses.
• Necessary contact lenses are contact lenses that are prescribed by your provider for other than
elective or cosmetic purposes. Necessary contact lenses are used to treat specific conditions for which
contact lenses provide better visual correction.
When you see a VSP Choice network provider:
• The plan pays up to $150 for elective contacts. You pay a $30 copay when you receive contact lens
evaluation and fitting exam at the time of service. You also pay any amount over $150.
• The plan pays 100 percent of the allowed amount for necessary contact lenses. You pay a $30 copay
when you receive contact lens evaluation and fitting exam at the time of service.
When you see an out-of-network provider you pay 100 percent of the billed charges. When you submit a
claim, VSP will reimburse you up to the following amounts:
• $105 for elective contacts including any fitting/evaluation services
• $210 for necessary contact lenses including any fitting/evaluation services
When you receive services from outside the country you pay 100 percent of the billed charges. When you
submit a claim, VSP will reimburse you up to the following amounts:
• $150 elective contacts including any fitting/evaluation services
2024 UMP CDHP (PEBB) Certificate of Coverage 83
• $150 necessary contact lenses including any fitting/evaluation services
Low vision benefit
The plan covers low vision benefits when vision loss is sufficient enough to prevent reading and
performing daily activities with standard corrective eyewear. If you fall within this category, you are
entitled to professional services, as well as ophthalmic materials. These services and equipment are
subject to the limitations stated below. Contact your VSP Choice network provider for more information.
You pay 25 percent of the allowed amount for covered supplemental aids. The plan pays 75 percent of the
allowed amount for medically necessary supplemental aids provided by VSP choice network providers and
out-of-network providers. When you see an out-of-network provider for covered supplemental aids, you
pay 100 percent of the billed charges. VSP will reimburse you up to 75 percent of the allowed amount
when you submit a claim for covered aids.
The maximum low vision benefit available is $1,000 (excluding your coinsurance) every two calendar years
for supplemental examinations (testing) and supplemental aids combined when provided by VSP Choice
network providers and out-of-network providers. There is a benefit maximum of two supplemental
examinations (testing) and all supplemental aids combined.
Supplemental examinations (testing)
You may receive up to two medically necessary supplemental tests (complete low vision analysis and
diagnosis), including a comprehensive examination of visual functions, and the prescription of corrective
eyewear or low vision aids when noted by the provider every two calendar years. When you see a VSP
Choice network provider, you pay $0 and the plan pays 100 percent of the allowed amount. When you
see an out-of-network provider you pay 100 percent of the billed charges. VSP will reimburse you up to
$125 when you submit a claim for covered services.
Supplemental aids
The plan pays for covered supplemental aids every two calendar years, which may include:
• Optical and non-optical aids; and
• Training on how to use the aids.
Children (under age 19)
ALERT! Out-of-network providers are not covered for any routine vision services.
The below VSP coverage table applies to children under age 19.
Benefit
Frequency
Your cost with a VSP
Choice network provider
Your cost with an out-of-
network provider
Professional
comprehensive
routine eye
exams
One per calendar
year.
You pay $0 of the allowed
amount and the plan pays
100% of the allowed
amount.
You pay 100% of billed
charges.
Frames
One per calendar
year.
You pay $0 of the allowed
amount and the plan pays
100% of the allowed
amount.
You pay 100% of billed
charges.
84 2024 UMP CDHP (PEBB) Certificate of Coverage
Benefit
Frequency
Your cost with a VSP
Choice network provider
Your cost with an out-of-
network provider
Lenses and
enhancements
One set per calendar
year.
You pay $0 for the
following covered lenses
and the plan pays 100% of
the allowed amount:
• Single vision lenses
• Lined bifocal lenses
• Standard progressive
lenses
• Lined trifocal lenses
• Lenticular lenses
You pay $0 for the
following lens
enhancements and the plan
pays 100% of the allowed
amount:
• Scratch-resistant coating
• Ultraviolet (UV)
protected lenses
• Impact-resistant coating
You pay 100% of billed
charges.
Contacts
One set of contact
lenses or disposable
contact lenses up to
the maximum
allowance instead of
frames and lenses
every calendar year.
You pay $0 of the allowed
amount for elective or
necessary contact lenses
and the plan pays 100% of
the allowed amount.
You pay $0 of the allowed
amount for contact lens
evaluation and fitting exam
and the plan pays 100% of
the allowed amount.
You pay 100% of billed
charges.
Note: Walmart®, Sam’s Club®, and Costco® providers are not VSP Choice network providers for children
under age 19 for frames, lenses, and contact lenses. Call VSP Member Services at 1-844-299-3041 for out-
of-network plan details or TTY 1-800-428-4833.
Vision exam
You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount when you see a
VSP Choice network provider for one professional comprehensive routine eye examination with refraction
or visual analysis per calendar year, including:
• Prescribing and ordering proper lenses;
• Verifying the accuracy of the finished lenses; and
• Progress or follow-up work as necessary.

2024 UMP CDHP (PEBB) Certificate of Coverage 85
Vision hardware
Lenses for glasses
You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount when you see a
VSP Choice network provider once every calendar year for one set of covered glass or plastic lenses.
Frames
You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount for one covered
frame every calendar year when you see a VSP Choice network provider.
Contact lenses
• You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount for elective
contact lenses or necessary contact lenses in lieu of frames and lenses once every calendar year when
you see a VSP Choice network provider.
• You pay $0 and the plan pays 100 percent of the allowed amount for contact lens evaluation and fitting
exam when you see a VSP Choice network provider.
Low vision benefit
ALERT! Out-of-network providers are not covered for any low vision services.
The plan covers low vision benefits when vision loss is sufficient enough to prevent reading and
performing daily activities with standard corrective eyewear. If you fall within this category, you are
entitled to professional services, as well as ophthalmic materials at no cost to you when the services are
provided by a VSP Choice network provider. These services and equipment are subject to the limitations
stated below. Contact your VSP Choice network provider for more information.
Supplemental examinations (testing)
You may receive up to two medically necessary supplemental tests (complete low vision analysis and
diagnosis), including a comprehensive examination of visual functions, and the prescription of corrective
eyewear or low vision aids when noted by the provider every two calendar years when you see a VSP
Choice network provider.
Supplemental aids
The plan pays for covered supplemental aids every two calendar years, which may include:
• Optical and non-optical aids; and
• Training on how to use the aids.
Vision claims administration
This section explains how VSP administers claims.
How to submit a vision claim for reimbursement
When you visit a VSP Choice network provider, the doctor will submit the claim directly to VSP for
payment.
If you are a member and are age 19 or older and you see an out-of-network provider, you pay 100
percent of the billed charges. You can submit the claim online or by mail. See the Directory pages at the
beginning of this booklet for links and contact information.
86 2024 UMP CDHP (PEBB) Certificate of Coverage
When you submit a claim, attach an itemized receipt that includes the following information:
• Doctor’s name or office name;
• Name of patient;
• Date of service; and
• Each service received and the amount paid.
Timely submitting of claims
You have 12 months from the date of service to submit your claim. If you do not submit your claim within
12 months of the date of service, it will be denied.
If you disagree with how your claim was processed, you may file a complaint or an appeal.
Vision complaints and appeals
How to submit a vision complaint
Complaints can be submitted through a written or verbal request. See the Directory pages at the
beginning of this booklet for links and contact information.
How to submit a vision appeal
You have the right to appeal if:
• You do not agree with VSP's decision about your health care.
• VSP will not approve or give you care you feel it should cover.
• VSP is stopping care you feel you still need.
VSP normally has 30 days to process your appeal. In some cases, you have a right to an expedited appeal.
You can get an expedited appeal if your health or ability to function could be seriously harmed by waiting
30 days for a standard appeal. If you ask for an expedited appeal, VSP will decide whether your request is
approved. If not approved, your appeal will be processed in 30 days. If any doctor asks VSP to give you an
expedited appeal, or supports your request for an expedited appeal, it must be given to you.
If you want to file an appeal which will be processed within 30 days, do the following:
File the request in writing with VSP. See the Directory pages at the beginning of this booklet for contact
information. Your appeal request will be processed within 30 days from the date your request is received.
If you want to file an expedited appeal, which will be processed within 24 hours, do the following:
• File an oral or written request for an expedited appeal. Specifically state that "I am requesting an
expedited appeal," or "I believe that my health could be seriously harmed by waiting 30 days for a
normal appeal."
• To file a request orally, call VSP Member Services. VSP will document the oral request in writing.
See the Directory pages at the beginning of this booklet for contact information.
Help with your appeal:
If you decide to appeal and want help with your appeal, you may have your doctor, a friend, lawyer, or
someone else help you. There are several groups that can help you. If you are covered by Medicare, you
may contact the Medicare Rights Center toll free at 1-888-466-9050 (TRS: 711). You may also contact the
National Institute on Aging at 1-800-222-2225 (TRS: 711) to request the phone number of your local Area
Agency on Aging or Health Insurance Counseling and Assistance Program (HICAP).

2024 UMP CDHP (PEBB) Certificate of Coverage 87
Your prescription drug benefit
See the Directory for prescription drug contact information.
Your plan’s prescription drug benefit is managed by a partnership of companies known as Washington
State Rx Services (WSRxS):
• Preauthorization, appeals, and customer service: Moda Health
• Network mail-order pharmacies:
▪ Costco Mail-Order Pharmacy
▪ Postal Prescription Services (PPS)
▪ Note: The plan does not cover prescription drugs purchased through mail-order pharmacies located
outside the U.S.
• Network specialty drug pharmacy: Ardon Health
Visit the UMP Prescription drug coverage webpage to:
• Find a link to the UMP Preferred Drug List and the Drug Price Check tool.
• Find a link to your online pharmacy account.
• Find information on mail-order and specialty drugs.
• Learn about submitting prescription drug claims.
• Locate network pharmacies or network vaccination pharmacies.
• Review prescription drug policies and programs.
Contact the mail-order or specialty drug pharmacy directly for help placing or tracking prescription
orders. If additional help is needed, contact WSRxS Customer Service.
Note: Regence BlueShield does not provide prescription drug benefits for UMP. Always contact WSRxS
with questions about your prescription drug coverage.
TIP: The UMP Preferred Drug List is available on the UMP Prescription drug coverage webpage
(see Directory for link). On this webpage, you will also find a link to the Drug Price Check tool
(the prices for drugs listed in this tool assume you have met your deductible).
The UMP Preferred Drug List
The UMP Preferred Drug List (sometimes called a “formulary”) lists all of the preferred drugs that UMP
covers. Drugs not listed on the Preferred Drug List are not covered unless an exception is requested and
approved by UMP. Excluded prescription drugs and products are not eligible for an exception. For the
exception process, refer to “Requesting an exception for noncovered prescription drugs” on page 89. The
UMP Preferred Drug List includes:
• If the plan must preauthorize a prescription drug (see page 98)
• If you must purchase a prescription drug from the plan’s network specialty drug pharmacy (see page
99)
• If there are any limits on a prescription drug’s coverage (see the "Limits on your prescription drug
coverage" section)
88 2024 UMP CDHP (PEBB) Certificate of Coverage
• If there are less expensive alternatives
The UMP Preferred Drug List is updated online throughout the year, and how a prescription drug is
covered may change at any time. You may look up your prescription drugs online on the UMP
Prescription drug coverage webpage or by contacting WSRxS. New brand-name prescription drugs may
not be covered during the first 180 days they are available. To check if a new prescription drug is covered,
contact WSRxS Customer Service.
Preferred drugs
Preferred drugs, including preferred specialty drugs, have been reviewed by the Washington State
Pharmacy and Therapeutics (P&T) Committee or by WSRxS and found to be safe and clinically effective
when compared to other drugs in the same therapeutic class or category. HCA or WSRxS has found these
drugs to be among the most cost-effective drugs for their therapeutic class or category due to their
favorable pricing.
Noncovered prescription drugs
Noncovered prescription drugs are not covered unless a Preferred Drug List exception is requested and
approved (see “Requesting an exception for noncovered prescription drugs”). These prescription drugs
have been reviewed by the Washington State Pharmacy and Therapeutics (P&T) Committee or WSRxS.
HCA or WSRxS has found these drugs are not as cost-effective and do not have a clinically significant
therapeutic advantage over the Preferred Drug List alternative(s).
ALERT! When a generic equivalent for a brand-name prescription drug becomes available, the
brand-name drug immediately becomes noncovered. An exception must be requested and
approved for coverage of the brand-name drug if you want to continue using the brand-name
drug. Always ask your provider to allow substitution on your prescriptions to save you money.
See the “Substitution under Washington State law” section for more information on
transitioning from a brand-name to generic prescription drug.
Requesting an exception for noncovered prescription drugs
ALERT! The UMP Preferred Drug List may not show every alternative prescription drug you
must try before an exception may be granted. If your exception request is denied, the plan’s
response letter will include the reason for the denial and the steps you can take next.
If you are prescribed a noncovered drug, and you have tried all the alternative drugs and none are found
to be effective, or if the alternatives are found to not be medically appropriate, you or your prescribing
provider can request an exception by contacting WSRxS Customer Service.
Your prescribing provider can also use CoverMyMeds to request an exception. CoverMyMeds is a free
online platform that reviews exception requests from electronic health record systems or directly through
the CoverMyMeds portal. To get started, have your provider visit the CoverMyMeds website (see Directory
for link).
Your prescribing provider must submit clinical information to request an exception. When the plan
approves an exception based on the criteria below, you will pay 15 percent of the drug’s cost per 30-day
supply after you pay your deductible, except for noncovered insulins. For noncovered insulins, when the

2024 UMP CDHP (PEBB) Certificate of Coverage 89
plan approves an exception based on the criteria below, you will pay the Tier 2 cost share (30 percent of
the allowed amount, $35 maximum payment per 30-day supply.
If your exception request is denied, the plan’s response letter will include the reason for the denial and the
steps you can take next.
Preferred drug list exceptions and coverage determinations are based on medical necessity. Because
requesting a noncovered drug exception requires medical information, only your prescribing provider
may submit clinical information for review. The prescribing provider will need to provide WSRxS with the
following information:
• The prescribing provider’s contact information;
• An explanation of why the plan should grant an exception;
• An explanation of how the requested medication therapy is evidence-based and generally accepted
medical practice;
• Documentation of medical necessity for the requested prescription drug over all other preferred
therapeutic alternatives; and
• At least one of the following items must also be included with the exception request:
▪ Confirmation and documentation from your prescribing provider that all preferred therapeutic
alternatives were tried for a clinically appropriate duration of treatment and failed to produce a
therapeutic response. If the requested exception is for a brand-name prescription drug that has an
FDA-approved generic equivalent, your prescribing provider must document your inadequate
response to at least two manufacturers of the generic drug, or to all manufacturers of the generic
drug if there are fewer than two manufacturers, in addition to all other preferred therapeutic
alternatives, before an exception is granted; or
▪ Confirmation and documentation from your prescribing provider that all preferred therapeutic
alternatives, including the required number of manufacturers of the same generic prescription drug,
caused an adverse drug reaction that prevents you from taking the prescription drug as directed. If
the requested exception is for a brand-name prescription drug that has an FDA-approved generic
equivalent, your prescribing provider must document your adverse drug reaction to at least two
manufacturers of the generic drug, or to all manufacturers of the generic drug if there are fewer than
two manufacturers, in addition to all other preferred therapeutic alternatives, before an exception is
granted.
ALERT! The exception process for noncovered drugs cannot be used for drugs that UMP
excludes. For more information about drugs UMP excludes, see the “Prescription drugs and
products UMP does not cover” and the “What the plan does not cover” sections.
How UMP decides which prescription drugs are preferred
Washington State P&T Committee and WSRxS P&T Committee provide recommendations to HCA. WSRxS
and HCA review the recommendations and determine which medications are included on the UMP
Preferred Drug List, as well as the tier level. The UMP Preferred Drug List includes the committees’
coverage recommendations.
Not all prescription drug classes are reviewed by the Washington State P&T Committee. For these
prescription drugs, the WSRxS P&T Committee makes coverage recommendations for HCA’s review and
final determination of a drug’s coverage.

90 2024 UMP CDHP (PEBB) Certificate of Coverage
For the plan to cover a prescription drug for you, it must be medically necessary for your health condition.
Your provider may prescribe a drug or drug dosage that does not meet the plan’s definition of medically
necessary and therefore will not be covered.
ALERT! A prescription drug may be noncovered even if no generic equivalent is available.
Guidelines for prescription drugs UMP covers
To be covered, a prescription drug must meet all of the following:
• Is listed on the UMP Preferred Drug List (The Preferred Drug List is subject to change).
• Does not have a nonprescription alternative, including an over-the-counter alternative with similar
safety, effectiveness, and ingredients.
• Has been dispensed from a licensed pharmacy employing licensed, registered pharmacists.
• Has been prescribed by a provider with prescribing authority within their scope of license.
• Has been reviewed by either the Washington State or WSRxS P&T Committee (see the "How UMP
decides which prescription drugs are preferred" section).
• Is approved by the FDA.
• Is medically necessary.
• Is not classified as a vitamin, mineral, dietary supplement, homeopathic drug, or medical food.
• Is not a noncovered prescription drug or product, unless an exception is granted.
• Is not an excluded prescription drug or product.
• May be legally obtained in the U.S. only with a written prescription.
• Meets plan coverage criteria.
The plan may cover FDA-approved prescription drugs for off-label use (prescribed for a use other than its
FDA-approved label) only if they are not excluded, the use is not considered experimental or
investigational by WSRxS, and the use is recognized as effective for treatment:
• In a standard reference compendium and supported by peer-reviewed clinical evidence; or
• In most relevant peer-reviewed medical literature, if not recognized in a standard reference
compendium; or
• By the federal Secretary of Health and Human Services.
Note: The plan may require that you try standard treatment(s) before it covers a prescription drug for off-
label use (prescribed for a use other than its FDA-approved label).
The plan will not cover any prescription drug when the FDA has determined its use to be unsafe.
ALERT! The plan does not cover prescription drugs purchased through mail-order pharmacies
located outside the U.S.
2024 UMP CDHP (PEBB) Certificate of Coverage 91
Nonprescription drugs and supplies
If you are prescribed a noncovered prescription drug not listed on the UMP Preferred Drug List, you may
request an exception. For the exception process, refer to “Requesting an exception for noncovered
prescription drugs” on page 89.
Your prescription drug benefit also includes the following nonprescription drugs and supplies:
• FDA-approved over-the-counter contraceptives. For the plan to cover FDA-approved over-the-counter
contraceptives, you must present your UMP member ID card and make your purchase at the pharmacy
counter. When possible, get a prescription, as not all pharmacies have prescribing authority. If you go
to a pharmacy without a prescription and the pharmacy does not have prescribing authority, you will
need to submit a claim to WSRxS.
• Diabetes care supplies, such as test strips, lancets, insulin syringes, and continuous glucose monitors
used in the treatment of diabetes. See the “Diabetes care supplies” benefit for more information.
• Other over-the-counter products that are specifically noted in the UMP Preferred Drug List as covered
by the plan.
• Each month, up to two over-the-counter COVID test kits will be covered as described in the UMP
Preferred Drug List
Products covered under the preventive care benefit
ALERT! For products covered as preventive — even if normally available over-the-counter
without a prescription — you must have a prescription and buy it at the pharmacy counter in a
network pharmacy to receive 100 percent reimbursement. You may not receive full
reimbursement for claims from non-pharmacy register receipts and non-network pharmacies.
Prescriptions purchased from an excluded pharmacy will not be covered. See the definition of
“Excluded pharmacy.”
Some products are covered under the preventive care benefit if they:
• Are recommended by the U.S. Preventive Services Task Force and the Advisory Committee on
Immunization Practices of the Centers for Disease Control and Prevention (see the “Preventive care”
benefit); and
• Conform to coverage guidelines (see the "How UMP decides which prescription drugs are preferred"
section).
The brands and types of products covered are limited. For a list of covered preventive care products,
check the Preferred Drug List, or contact WSRxS Customer Service. You pay $0 if your provider writes you
a prescription and you purchase these products from the pharmacy counter at a network pharmacy. If you
purchase over-the-counter and send in a paper claim, you may pay part of the cost.
Contraceptive drugs and supplies are covered as preventive (see the “Family planning services” benefit for
details). See the “Tobacco cessation services” benefit for products covered as preventive for tobacco
cessation.
Injectable drugs available under the pharmacy benefit
Certain injectable drugs may only be available through your pharmacy benefit. You can check the UMP
Preferred Drug List to see if an injectable drug is covered through your pharmacy benefit. Some injectable
drugs may need to be administered by a health care provider, and these drugs are typically available
92 2024 UMP CDHP (PEBB) Certificate of Coverage
through your medical benefit. Vaccines administered at network pharmacies may be covered under your
pharmacy benefit.
Compounded prescription drugs
Compounded prescription drugs are the result of combining, mixing, or altering ingredients by a
pharmacist in response to a physician’s prescription to create a new drug tailored to the specialized
medical needs of an individual member. Traditional compounding typically occurs when an FDA-approved
prescription drug is unavailable, or a licensed health care provider decides that an FDA-approved drug is
not appropriate for a member’s medical needs. Compounded prescription drugs require preauthorization.
Claims for compounded drugs require additional information submitted on the claim form. This
information is available from the compounding pharmacy.
What you pay for prescription drugs
ALERT! Hospice care: See page 55 for special prescription drug coverage while in hospice.
You will pay the entire cost of your medical services and prescription drugs until you meet your
deductible. Covered preventive drugs, covered insulin, and certain other drugs as indicated on the UMP
Preferred Drug List are not subject to your deductible. Once you have met your deductible, you pay 15
percent of the allowed amount for covered prescription drugs when purchased through a network
pharmacy up to your out-of-pocket limit. Once you reach your out-of-pocket limit, the plan pays 100
percent of the allowed amount for covered prescription drugs at a network pharmacy. You may purchase
up to a 90-day supply for most prescription drugs. For most specialty drugs, you may purchase up to a
30-day supply. You pay $0 for covered preventive drugs when you use a network pharmacy.
Covered Insulins
For covered insulins, you must fill your prescription at a network pharmacy to pay the appropriate cost-
share, even if you have not met your deductible. If you have not met your deductible, your cost-share will
be applied to your deductible. See the table below for how much you will pay for covered insulins when
you fill your prescription at a network pharmacy.
Tier and description
How much you pay for covered insulins
All network pharmacies (retail and mail-order)
Value Tier (Value)
• 0–30-day supply:
▪ 5% coinsurance or $10, whichever is less
• 31–60-day supply:
▪ 5% coinsurance or $20, whichever is less
• 61–90-day supply:
▪ 5% coinsurance or $30, whichever is less
Tier 1 (Tier 1)
• 0–30-day supply:
▪ 10% coinsurance or $25, whichever is less
• 31–60-day supply:
▪ 10% coinsurance or $50, whichever is less
2024 UMP CDHP (PEBB) Certificate of Coverage 93
Tier and description
How much you pay for covered insulins
All network pharmacies (retail and mail-order)
• 61–90-day supply:
▪ 10% coinsurance or $75, whichever is less
Tier 2 (Tier 2)
• 0-30 day-supply:
▪ 30% coinsurance or $35, whichever is less
• 31–60 day-supply:
▪ 30% coinsurance or $70, whichever is less
• 61–90 day-supply:
▪ 30% coinsurance or $105, whichever is less
To check your cost, do either of the following:
• Use the Drug Price Check tool on the UMP Prescription drug coverage webpage (the prices for drugs
listed in this tool assume you have met your deductible).
• Contact WSRxS Customer Service.
See the Directory pages at the beginning of this booklet for link and contact information.
If a prescription drug is not covered by the plan, it does not apply to your deductible or your out-of-
pocket limit.
Note: You may use your HSA to pay for many prescription drugs not covered by the plan. See the “Health
savings account (HSA)” section for more information.
Note: You must use UMP’s network mail-order pharmacies to fill mail-order prescriptions. If you use any
other mail-order service to fill your prescription drugs, or you purchase them outside of the U.S., the plan
will not cover these drugs if UMP is your primary plan.
ALERT! When you use network pharmacies, retail or mail-order, you pay based on the
prescription drug’s allowed amount, a discounted price negotiated with the plan. If you use a
non-network pharmacy, the pharmacy may charge more than the allowed amount. You will
have to pay this additional amount, which does not apply to your deductible or out-of-pocket
limit.
If you have other prescription drug coverage
If you have primary medical coverage through another plan that covers prescription drugs, some of the
limits and restrictions to prescription drug coverage listed on page 121 will apply when UMP pays
secondary to another plan. See the “Submitting a claim for prescription drugs” section for how to submit
your prescription drug claim.
Using network pharmacies when UMP is secondary
If you have primary coverage through another plan that covers prescription drugs, show both plan cards
to the pharmacy and make sure they know which plan is primary. It is important that the pharmacy bills
the plans in the correct order, or claims may be denied or paid incorrectly.

94 2024 UMP CDHP (PEBB) Certificate of Coverage
Using mail-order pharmacies when UMP is secondary
If your primary plan uses UMP’s network mail-order pharmacies, these pharmacies may process payments
for both plans and charge you only what is left. Make sure that UMP’s network mail-order pharmacies
have your information for both plans and know which plan is primary.
However, if your primary plan uses a different mail-order pharmacy, you will have to use your primary
plan’s mail-order pharmacy, then submit a paper claim for payment by UMP. See the “Submitting a claim
for prescription drugs” section for how to do this.
Where to buy your prescription drugs
ALERT! If you use a non-network retail pharmacy, you will pay the entire cost of the
prescription drug at the time of purchase and must submit a claim for reimbursement.
However, only the allowed amount for covered drugs will apply to your deductible or out-of-
pocket limit, if applicable. Prescriptions purchased from an excluded pharmacy are not covered.
Pharmacies are contracted through a different network than medical providers.
Retail pharmacies
WSRxS has a large national network of retail pharmacies, which includes many independent and regional
pharmacies in Washington State, as well as national chains. Search for a network pharmacy on the UMP
Prescription drug coverage webpage or contact WSRxS Customer Service (see Directory for link and
contact information).
When you get your prescriptions at a network pharmacy, the pharmacy sends the claim to the plan for
you, and you pay only your cost-share (coinsurance and deductible) as described in the “What you pay for
prescription drugs” section. Covered insulin prescriptions filled at network pharmacies are not subject to
your deductible.
Note: You will pay the entire cost for any prescription drug not covered by the plan, which does not apply
to your deductible or your out-of-pocket limit.
TIP: If you take a prescription drug regularly, you may be able to save money by filling up to a
90-day supply at a network retail pharmacy or through UMP’s network mail-order pharmacies.
Search for a network pharmacy and compare prices on the UMP Prescription drug coverage
webpage.
Network vaccination pharmacies
Many network retail pharmacies have vaccination pharmacists who may give covered preventive
immunizations at no cost to you. Contact a network pharmacy ahead of time to make sure the pharmacy
has the vaccine you need. Present your UMP member ID card at the pharmacy counter before receiving a
vaccine.
2024 UMP CDHP (PEBB) Certificate of Coverage 95
Mail-order pharmacies: Costco Mail-Order Pharmacy and
Postal Prescription Services (PPS)
ALERT! UMP’s network mail-order pharmacies cannot ship outside of the U.S. See “Travel
overrides for prescription drugs” on page 101 if you will be traveling.
Costco Mail-Order Pharmacy and PPS are the plan’s only network mail-order pharmacies. Prescriptions
purchased through other mail-order pharmacies will not be covered if UMP is your primary plan. For
more information about mail-order, visit the UMP Prescription drug coverage webpage, contact UMP’s
network mail-order pharmacies, or contact WSRxS Customer Service. See the Directory pages at the
beginning of this booklet for links and contact information.
Note: You may mail in a prescription, however only a provider can call, fax, or electronically submit a
prescription to the pharmacy. You must follow these instructions to avoid a delay in filling your
prescription.
ALERT! The plan does not cover other mail-order pharmacies outside of UMP’s network mail-
order pharmacies if UMP is your primary insurance. If UMP is your secondary insurance, you
may use another mail-order pharmacy.
Refills may be ordered through UMP’s network mail-order pharmacies. When using UMP’s network mail-
order pharmacies, the same deductible, coinsurance, preauthorization requirements, and limits on
coverage apply as for prescription drugs purchased at retail network pharmacies.
ALERT! Drugs can be expensive. If you are not able to be home to receive the drug in the mail,
it may be a good idea to request that it be sent with a requirement for a signature, or find an
alternate point of delivery to ensure the package is not stolen. The plan is not responsible for
replacement of lost, stolen, expired, or damaged prescription drugs or products (see the “What
the plan does not cover” section).
Prescriptions mailed, or orders placed in December but not filled until January 1 or after, are subject to
your deductible applicable on the date the prescription is processed. Because of increased volume at the
end of the year, prescriptions submitted to the network mail-order pharmacies in December may not be
processed during the current plan year.
If there is a shortage of a specific prescription drug that UMP’s network mail-order pharmacies cannot
control, and it does not have the quantity you ordered, the network mail-order pharmacies will contact
you to discuss your options for obtaining your prescription(s).
ALERT! Some Durable Medical Equipment (DME) items are not available through UMP’s
network mail-order pharmacies. You will need to get them through a network retail pharmacy
or preferred DME provider.

96 2024 UMP CDHP (PEBB) Certificate of Coverage
How to get the plan discount
Be sure to fill your prescriptions at a network pharmacy and show your ID card at the pharmacy counter. If
you do, you pay for covered prescription drugs based on the allowed amount (WSRxS’ standard
reimbursement). If you do not show your UMP member ID card at a network pharmacy or you use a non-
network pharmacy, then you may be charged a higher amount. If the amount charged is more than the
UMP allowed amount, you will pay the difference in addition to your coinsurance. Prescriptions purchased
from an excluded pharmacy are not covered.
If you have more than one insurance plan and UMP is your secondary insurance, show both plan member
ID cards at the pharmacy and make sure they know which plan pays first so the pharmacy may bill the
plans in the correct order.
Non-network pharmacies: Retail
You will save money when you buy your prescriptions at network retail pharmacies and network mail-
order pharmacies. You may buy your prescriptions (except specialty drugs) at a non-network retail
pharmacy, but you will pay more if you do. If you get your prescriptions filled at a non-network retail
pharmacy, the following applies:
• You need to submit your claim to WSRxS for reimbursement (see the “Submitting a claim for
prescription drugs” section).
• You do not get the plan discount.
• You will pay the difference between the allowed amount and what the pharmacy charges, and it will
not apply to your deductible or out-of-pocket limit. Claims for covered insulins must be submitted to
WSRxS for reimbursement before they can apply to your deductible.
• What the plan pays is based on the allowed amount for prescription drugs covered by the plan,
whether from a network or non-network retail pharmacy.
• Non-network pharmacies will not know if a prescription drug must be preauthorized, has a quantity
limit, or has other coverage limits. If you purchase a drug from a non-network pharmacy and limits
apply, the plan may not cover or reimburse it.
• Prescriptions purchased from an excluded pharmacy will not be covered. See the definition of
“Excluded pharmacy.”
• Specialty drugs must be purchased from the plan’s network specialty drug pharmacy. See the “Specialty
drug” section on page 99.
TIP: To submit claims for prescriptions purchased from non-network pharmacies (U.S. retail or
international retail pharmacies), see the “Submitting a claim for prescription drugs” section.
Prescription drugs purchased outside the U.S.
If you purchase prescription drugs outside the U.S. for any reason, the following rules apply:
• If the prescription drug is available only by prescription in the U.S. but does not require one outside the
U.S., the drug is covered only if prescribed by a provider practicing within their scope of practice.
• If you get a prescription drug that is approved for use in another country but not in the U.S., the plan
will not cover it.
2024 UMP CDHP (PEBB) Certificate of Coverage 97
• If you get a prescription drug that is available over-the-counter in the U.S., the plan will not cover the
drug, even if you have a prescription from a provider prescribing within their scope of practice. The
plan does not cover most over-the-counter drugs.
• If you get a prescription drug that is not covered by UMP, the plan will not pay any amount of the cost
of the drug. You will be responsible for the full cost of the drug.
To submit a claim for a prescription drug purchased at retail pharmacies outside the U.S., see the
“Submitting a claim for prescription drugs” section. All necessary information must be included on the
prescription drug claim form with drugs and dosage documented.
Limits on your prescription drug coverage
WSRxS may exclude, not cover, discontinue, or limit coverage for any prescription drug or manufacturer’s
version of a drug for any of the following reasons:
• A more cost-effective alternative is available to treat the same condition.
• A nonprescription alternative, including an over-the-counter alternative, becomes available.
• A prescription drug receives FDA approval for a new use.
• A prescription drug is used off label to treat an indication that is not determined to be medically
necessary by WSRxS.
• A prescription drug is purchased from an excluded pharmacy.
• Generic, biosimilar, interchangeable biosimilar, or follow-on biologic prescription drugs become
available.
• New prescription drugs are developed.
• The FDA denies, withdraws, or limits the approval of a prescription drug.
• The FDA’s Drug Efficacy Study Implementation (DESI) classifications finds a prescription drug to be less
than effective.
• The Washington State P&T Committee or WSRxS recommends a change (see the "How UMP decides
which prescription drugs are preferred" section).
• There is a sound medical reason.
• There is lack of scientific evidence that a prescription drug is as safe and effective as existing drugs
used to treat the same or similar conditions.
• There is new scientific evidence demonstrating a prescription drug has been found to be less safe or
effective than existing drugs to treat the same or similar conditions.
Using free prescription drug samples does not guarantee coverage or waive requirements for
preauthorization, step therapy, quantity limits, day supply limits, or other limitations.
Prescription drugs will only be covered if:
• They are not excluded by the plan, are listed on the UMP Preferred Drug List, and are medically
necessary for your health condition; or
• You received an exception to cover a noncovered drug
Although your provider may prescribe a prescription drug that is not considered medically necessary, the
above conditions must be met in order for a prescription drug to be covered.
The plan excludes experimental or investigational prescription drugs. You may be liable for all charges if
you receive prescription drugs or products that are determined to be experimental or investigational (see
98 2024 UMP CDHP (PEBB) Certificate of Coverage
the “What the plan does not cover” section). If you disagree with the plan’s determination, you have the
right to an appeal (see the “Complaint and appeal procedures” section for that process).
The limits and restrictions described in the “Limits on your prescription drug coverage” section help
WSRxS monitor drug usage, safety, and costs. These limits and restrictions may be added or removed
from prescription drugs at any time. You may find out if your prescription drug falls under any of these
limits and restrictions by checking the UMP Preferred Drug List on the UMP Prescription drug coverage
webpage or contacting WSRxS Customer Service (see Directory for link and contact information).
Risk Evaluation and Mitigation Strategies (REMS)
Risk Evaluation and Mitigation Strategy (REMS) is a drug safety program that the FDA can require for
certain prescription drugs with serious safety concerns to help make sure the benefits of the drug
outweigh its risks. REMS are designed to reinforce prescription drug use behaviors and actions that
support the safe use of that drug. While all drugs have labeling that describe possible risks, only a few
prescription drugs require a REMS. REMS are not designed to mitigate all the adverse events of a
prescription drug. These are communicated to health care providers in the drug’s prescribing information.
Rather, REMS focuses on preventing, monitoring, and/or managing a specific serious risk by informing,
educating, and/or reinforcing actions to reduce the frequency and/or severity of the event.
If the REMS program is not followed, the plan may not cover the restricted drug.
Preauthorizing prescription drugs
Preauthorization is a process that helps make sure that prescription drug benefits are administered as
designed and that plan members receive a drug therapy that is safe and effective for their conditions, and
provides the greatest value. Some prescription drugs require preauthorization to determine whether they
are medically necessary and meet all applicable coverage criteria, or the plan will not cover them. You may
find out if your prescription drug requires preauthorization by contacting WSRxS Customer Service or
checking the UMP Preferred Drug List on the UMP Prescription drug coverage webpage. See the Directory
pages at the beginning of this booklet for links and contact information. You and your prescribing
provider may also find the coverage criteria for your prescription drug by referring to the Washington
State Rx Services (Moda) preauthorization (UMP PEBB Plans) preauthorization requirements on forms and
publications at hca.wa.gov/ump-forms-pubs.
If your prescription drug requires preauthorization, your pharmacist or prescribing provider may initiate a
request through CoverMyMeds, a free online platform that accepts requests from electronic health
records, or directly through the CoverMyMeds Portal. To get started, your pharmacist or prescribing
provider can go to the CoverMyMeds website. They may also contact WSRxS Customer Service to request
it.
If you have an existing authorization from UMP for a brand-name drug, and a generic drug becomes
available, you may need to renew your authorization to continue filling the brand-name drug. However, if
you switch to the generic drug, a new preauthorization is not required until the existing authorization
expires.
Note: Prescription drugs covered under the medical benefit rather than the prescription drug benefit have
different rules for preauthorization. Contact UMP Customer Service for details.
Emergency fill
Emergency fill lets you get a limited quantity of certain prescription drugs while the plan processes your
preauthorization request. This option is only available when a delay could result in emergency care,
hospital admission, or a serious threat to your health or others in contact with you. Contact WSRxS
Customer Service for questions about which prescriptions drugs may qualify for emergency fills.

2024 UMP CDHP (PEBB) Certificate of Coverage 99
You must bring your prescription to a network pharmacy and state that you need an emergency fill while
the plan processes your preauthorization request. You pay 15 percent coinsurance after you pay your
deductible.
The plan will cover an emergency fill of up to a seven-day prescription drug supply.
If your preauthorization request is denied, you will pay the full cost of the prescription drug for any
quantity you receive after the emergency fill.
Emergency fill limits
The following limits still apply to emergency fill prescription drugs:
• Quantity limits: You cannot get more than the stated quantity limit under an emergency fill. If you have
a current filled prescription for a prescription drug (or its therapeutic equivalent) and it was filled to the
quantity limit, you cannot get an emergency fill until you have used 84 percent or more of the filled
prescription.
• Refill too soon: If you have a filled prescription for a prescription drug (or its therapeutic equivalent),
you cannot get an emergency fill until you have used 84 percent or more of the filled prescription.
Quantity limits
Certain prescription drugs have a per prescription limit on how much you get for each fill. If you need
more than this limit allows, your pharmacist or prescribing provider may initiate a request through
CoverMyMeds on the CoverMyMeds website or contact WSRxS Customer Service. See the Directory pages
at the beginning of this booklet for links and contact information.
If WSRxS denies your request or your provider or pharmacist does not get preauthorization, the plan will
cover the prescription drug only up to the quantity limit amount. You will pay for any extra amount.
Specialty drugs
ALERT! Specialty drugs can be expensive. If you are not able to be home to receive the drug in
the mail, it may be a good idea to request that it be sent with a requirement for a signature, or
find an alternate point of delivery to ensure the package is not stolen.
Specialty drugs are high-cost injectable, infused, oral, or inhaled prescription drugs or products that
require special handling and storage and are subject to additional rules. You may find out if a drug is a
specialty drug by checking the UMP Preferred Drug List on the UMP Prescription drug coverage webpage,
or by contacting WSRxS Customer Service. See the Directory pages at the beginning of this booklet for
links and contact information.
Specialty drugs are covered only when purchased through the plan’s network specialty drug pharmacy. If
that pharmacy does not have access to a specialty drug, you will be notified to fill your prescription at
another specialty pharmacy. If the network specialty pharmacy gains access to the specialty drug, you will
receive notification to transfer your prescription to that pharmacy.
You may receive up to a 30-day supply for most specialty prescription drugs per prescription or refill.
However, some may be limited to a 15-day supply due to high discontinuation rate, short duration of use,
or to make sure that the prescription drug is not causing harmful side effects.
Specialty drugs require preauthorization. See “Preauthorizing prescription drugs” on page 98 for how to
request preauthorization. A patient care coordinator will work with you to schedule a delivery time for the
prescription drug. The specialty drug pharmacy will deliver your prescription drugs anywhere in the U.S.

100 2024 UMP CDHP (PEBB) Certificate of Coverage
that you choose, such as to your workplace or to a neighbor if you cannot be home for the delivery.
Specialty prescription drugs often require special handling and storage. The plan is not responsible for
replacement of lost, stolen, expired, or damaged prescription drugs or products (see the “What the plan
does not cover” section).
If your provider will be administering the prescription drug, you may have it shipped to the provider’s
office. However, once the provider’s office receives the prescription drug, the provider takes responsibility
for it.
The plan’s network specialty drug pharmacy cannot ship outside the U.S. See “Travel overrides for
prescription drugs” on page 101 if you will be traveling.
Step therapy
When a prescription drug is part of the step therapy program, you have to try certain drugs (Step 1)
before the plan will cover the prescribed (Step 2) drug. When a prescription for a step therapy drug is
submitted “out of order,” meaning you have not first tried the Step 1 drug before submitting a
prescription for a Step 2 drug, the plan will not cover your prescription. When this happens, your provider
will need to prescribe the Step 1 drug for you.
If you or your provider feels that you need the Step 2 prescription filled as originally written without first
trying the Step 1 drug, your pharmacist or prescribing provider may contact WSRxS Customer Service and
request coverage. You will have to pay the entire cost of the prescription drug if you have not tried the
Step 1 drug and coverage has not been authorized before you get the Step 2 drug.
To find out if step therapy applies to your drug, check the UMP Preferred Drug List on the UMP
Prescription drug coverage webpage, or contact WSRxS Customer Service.
Note: Only network pharmacies will check to see if step therapy applies to your prescription drug. If you
get a step therapy drug at a non-network pharmacy, the plan may not cover the drug.
Substitution under Washington State law
ALERT! New generic prescription drugs are released throughout the year. If you want to save
money by using generics, ask your provider to allow substitution on your prescriptions, even if
a generic drug is not available now. That way, when one becomes available, the pharmacist
may automatically refill with the generic.
When a brand-name or biologic prescription drug has a generic equivalent or interchangeable biosimilar,
pharmacists in Washington State must substitute the generic equivalent or interchangeable biosimilar
drug for the brand-name or biologic prescription drug. When a generic equivalent for a brand-name
prescription drug becomes available, the brand-name drug immediately becomes noncovered.
Your provider may write the prescription “dispense as written” if they want you to get only the prescribed
brand-name or biologic prescription drug. Or you may tell the pharmacist you want the brand-name or
biologic drug. Regardless of whether you or your prescribing provider ask the pharmacist to “dispense as
written,” if you get the noncovered prescription drug, the plan may not cover it. Final determination of
medical necessity for FDA-approved contraceptives is determined by the attending prescribing provider.
To request an exception for a noncovered drug, see page 102.
2024 UMP CDHP (PEBB) Certificate of Coverage 101
Therapeutic Interchange Program
The Washington State Therapeutic Interchange Program allows a pharmacist to substitute a “therapeutic
alternative” drug for a noncovered drug in certain cases. Therapeutic alternatives are drugs that are
chemically different from your prescribed drug but provide the same therapeutic benefit.
You may find out if your prescription drug is affected by the Therapeutic Interchange Program by
checking the UMP Preferred Drug List on the UMP Prescription drug coverage webpage or by contacting
WSRxS Customer Service (see Directory for link and contact information). The Therapeutic Interchange
program does not affect all noncovered prescription drugs.
The pharmacist will substitute the preferred drug when your prescribing provider has “endorsed” the
Washington Preferred Drug List, and:
• You are filling your prescription in Washington State or through UMP’s network mail-order pharmacies.
• Your prescribing provider allows substitution on your prescription.
If you do not want your prescription drug to be changed, the plan may not cover your drug if you ask the
pharmacist to fill the prescription as written.
Regardless of whether you or your prescribing provider ask the pharmacist to “dispense as written,” if you
get the noncovered prescription drug, the plan may not cover it.
The pharmacy will contact your provider to request authorization for the substitution. If approved by the
provider, you will receive the alternative preferred drug along with a letter of explanation. If the pharmacy
cannot get an authorization from your provider within 48 hours, the prescription will be filled as written,
and you will be charged the full price of the drug.
Travel overrides for prescription drugs
You may request a travel override to get an extra supply of prescription drugs for extended travel. All of
the conditions listed below apply.
• You may request a travel override up to two weeks before your departure.
• You may request no more than two travel overrides per calendar year, including all travel within or
outside the U.S.
• Within the U.S., you may request up to a 90-day supply per prescription, or as allowed under that
prescription.
• Outside the U.S., you may request up to a six-month supply per prescription, or as allowed under that
prescription.
• Travel overrides will be granted only while you are covered by the plan. If your eligibility is ending, the
plan does not cover prescription drugs past the time your enrollment in the plan ends.
• You will pay applicable charges (deductible and coinsurance) for each extra supply received.
To request a travel override, contact WSRxS Customer Service.
Refill too soon
The plan will not cover a refill until 84 percent of the last prescription should be used up. Claims for
therapeutic equivalents of the previously prescribed drug will also be denied. This also applies if your
prescription is damaged, destroyed, lost, or stolen. For example, if you get a 90-day supply and you try to
refill this prescription before 76 days have passed, coverage will be denied.
However, in the event of an emergency or other urgent circumstance, you may request an exception to
override the refill too soon policy. The plan may require documentation to support your request. Approval
of your request is at the sole discretion of the plan.

102 2024 UMP CDHP (PEBB) Certificate of Coverage
Early refill for a natural disaster
You may request an early refill for your prescription when you need to evacuate for a natural disaster. To
request an early refill or to locate pharmacies that remain open near you, contact WSRxS Customer
Service.
What to do if the plan denies coverage
TIP: If your prescription coverage is denied by the pharmacy due to plan enrollment issues,
contact:
Employees: Your employer’s payroll, or benefits office.
Retirees, PEBB Continuation Coverage, and retired employees of a former employer
group: PEBB Program at 1-800-200-1004 (TRS: 711).
If a network pharmacy (including mail-order or specialty drug) tells you that preauthorization is required,
coverage is denied, or quantities are limited, you, your pharmacist, or your prescribing provider may
contact WSRxS Customer Service to request a coverage review or preauthorization.
If WSRxS denies the coverage request, you have the right to submit an appeal (see the “Complaint and
appeal procedures” section).
If your provider thinks you need the prescription drug immediately, they may request an expedited review
by submitting all clinically relevant information to the plan by phone or fax. An expedited appeal replaces
the first and second level appeals. WSRxS will decide on coverage of the prescription drug within 72 hours
of the request. In this case, you may choose to purchase a three-day supply at your own expense.
Prescription drugs and products UMP does not cover
Prescription drugs and products not covered under the prescription drug benefit include, but are not
limited to, noncovered prescription drugs and excluded drugs and products.
Noncovered prescription drugs
• Noncovered prescription drugs are not covered without an approved UMP Preferred Drug List
exception request
For more information, see the “Noncovered prescription drugs” section on page 88.
Excluded drugs and products
• Dental preparations, such as rinses and pastes.
• Dietary/food supplements, vitamins, minerals, herbal supplements, and medical foods.
• Experimental or investigational prescription drugs.
• Homeopathic drugs, including FDA-approved prescription products.
• Over-the-counter drugs, products containing an over-the-counter drug, or prescription drugs that have
a nonprescription alternative, except for the drugs specified under “Exceptions covered” on page 91, or
otherwise listed on the UMP Preferred Drug List.
Note: Prescription drugs with a nonprescription alternative — including an over-the-counter
alternative having similar safety, efficacy, and ingredients — are excluded.

2024 UMP CDHP (PEBB) Certificate of Coverage 103
• Over-the-counter products not approved by and registered with the FDA.
• Prescription drugs prescribed for excluded conditions.
• Prescription drug costs covered by other insurance (see page 121 for coordination with other plans).
• Prescription drugs not approved by the FDA.
• Prescription drugs provided to a member, in whole or in part, while the member is admitted to an
inpatient facility. Drugs provided in an inpatient setting are covered under the medical benefit.
• Prescription drugs that are not medically necessary.
• Prescription drugs that are repackaged.
• Prescription drugs that the FDA’s DESI classifications have found to be less than effective.
• Prescription drugs under a REMS program required by the FDA when prescribed outside REMS
guidelines (see page 98 for details).
• Most products considered as a medical device by the FDA. Medical devices may be covered under your
medical benefit.
The plan also excludes prescription drugs to treat conditions that are not covered under the medical
benefit. These include, but are not limited to, prescription drugs for:
• Cosmetic purposes.
• Fertility or infertility.
• Obesity (or weight loss).
• Promoting hair growth.
• Sexual dysfunction.
Limits on plan coverage
If you receive a service that is not medically necessary, is experimental or investigational, is listed as an
exclusion in the “What the plan does not cover” section, or is listed as a noncovered or excluded
prescription drug, you are responsible for paying all associated charges.
Preauthorizing medical services
ALERT! This section does not apply to prescription drugs. See page 98 for how to request
preauthorization of drugs covered under the prescription drug benefit.
The plan must preauthorize some medical services and supplies to determine whether the service or
supply meets the plan’s medical necessity criteria to be covered. The fact that a service or supply is
prescribed or furnished by a provider does not, by itself, make it a medically necessary covered
service. Preauthorization is not a guarantee of coverage.
A change after the plan has approved a preauthorization request — including, but not limited to, a
change of provider or different/additional services — requires your provider to submit a new
preauthorization request and for the plan to approve it.
If your preauthorization is denied, your provider may request a peer-to-peer review where they can talk to
a Regence BlueShield provider about your condition prior to submitting an appeal. For more information
contact UMP customer service.
104 2024 UMP CDHP (PEBB) Certificate of Coverage
Your preauthorization role
ALERT! Excluded, experimental, and investigational services do not require preauthorization
because they are not covered by the plan. To confirm whether a service is covered, contact
UMP Customer Service.
To be covered, some services, including, but not limited to, Applied Behavior Analysis (ABA) Therapy for
members age 18 or older (see page 40) and bariatric surgery (see page 41), must be preauthorized before
services are received. A preferred or participating provider may be required to request preauthorization
before providing services. Contact UMP Customer Service to ask if a service requires preauthorization and
how to submit a request.
An out-of-network provider is not obligated to obtain preauthorization for services that require a
preauthorization because they do not have a contract with Regence. If an out-of-network provider does
not obtain a required preauthorization in advance of the service, you will be responsible for all charges
billed to you.
You are encouraged to request that an out-of-network provider preauthorize certain services on your
behalf to determine medical necessity before the services are provided. They have the clinical details and
technical billing information needed to submit a request.
You may be liable for all charges if you receive services that are determined to be not medically necessary,
experimental or investigational, or not covered under this plan (see the “What the plan does not cover”
section).
ALERT! See the “Complaint and appeal procedures” section for how to appeal denial of a
preauthorization request before receiving services.
List of services and supplies requiring preauthorization or
notice
For a list of services and supplies requiring preauthorization or notice:
• Visit the UMP Policies that affect your care webpage.
• Contact UMP Customer Service to request a printed list or ask questions.
See the Directory pages at the beginning of this booklet for links and contact information.
ALERT! The UMP preauthorization list is updated throughout the year. The fact that a service
does not require preauthorization or notice does not guarantee coverage.
Notice for facility admissions
Your provider must notify the plan upon your admission to a facility for services requiring plan notice. You
may find a list of services requiring plan notice by visiting the UMP Policies that affect your care webpage
or contacting UMP Customer Service. Facility admissions for which the plan is not notified may not be

2024 UMP CDHP (PEBB) Certificate of Coverage 105
covered. Notice is usually done by the facility at the time you are admitted. Notice is not the same as
preauthorization and many services require both.
What is the difference between preauthorization and notice?
ALERT! Many services, including, but not limited to, inpatient services, require both
preauthorization and notice. Contact UMP Customer Service or talk to your provider if you
have questions about services needing preauthorization or notice.
“Preauthorization” is when your provider sends a request for coverage of a service on the UMP
preauthorization list. Preauthorization is usually requested by the provider performing the services. The
plan sends either an approval or denial of coverage.
If the plan does not approve services that require preauthorization before services are received, the plan
may deny coverage. The plan does not approve or deny preauthorization for services that are not on the
UMP preauthorization list.
“Notice” means that your provider must contact the plan to let us know when you receive services. Notice
is usually done by the facility when you are admitted.
ALERT! If the plan denies preauthorization and you receive those services anyway, you are
responsible for the provider’s entire billed charge.
How long the plan has to make a decision
The plan will respond to standard preauthorization requests submitted by contracted providers, within 5
days of receipt for non-electronic requests and within 3 days of receipt for electronic requests. For
expedited preauthorization requests, the plan will respond within 1 to 2 days of receipt. If additional
information is required, the plan will notify the provider within the timelines described in this section. You
will also be notified of the decision.
If your provider believes that waiting for a decision under the standard preauthorization timeline could
place your life, health, or ability to regain maximum function in serious danger, they can request an
expedited preauthorization request.
General information from UMP Customer Service
For services not requiring preauthorization, you may contact UMP Customer Service to ask if a particular
service is generally covered by the plan, and for an estimate of how much you will pay. The plan does not
approve or deny preauthorization for services that are not on the UMP preauthorization list.
Until a claim is submitted and reviewed, the plan cannot guarantee that your service will be covered or
give you an exact amount you will pay out of pocket. This is because when a provider bills for a service,
the plan pays for it based on procedure codes. Each code describes a service in some detail, and there are
many codes for similar-sounding services. Your provider, not the plan, determines which of these codes is
used on the submitted claim.
Alternative benefits
Alternative benefits mean benefits for services or supplies that are not otherwise covered as specified in
this COC, but for which the plan may approve coverage after case management evaluation. The plan may

106 2024 UMP CDHP (PEBB) Certificate of Coverage
cover alternative benefits through case management (see the “Care management” benefit) if the plan
determines that alternative benefits are medically necessary and will result in overall reduced covered
costs and improved quality of care.
Before alternative benefits are covered, the plan, you (or your legal representative), and, if required by the
plan, your physician or other provider, must enter into a written agreement of the terms and conditions
for payment. Alternative benefits are approved on a case-specific basis only. Approval of an alternative
benefit applies to only the services and member listed in the written agreement. The rest of this COC
remains in effect.
What the plan does not cover
TIP: If you have any questions about services the plan does not cover, contact UMP Customer
Service or WSRxS Customer Service.
This plan covers only the services and conditions specifically identified in this COC. Unless a service or
condition fits into one of the specific benefit definitions, it is not covered. You may pay all costs associated
with a noncovered service.
Here are some examples of common services and conditions that are not covered. Many others are also
not covered — these are examples only, not a complete list. These examples are called exclusions,
meaning these services are not covered, even if the services are medically necessary.
1. Activity therapy. The following activity therapy services include, but are not limited to:
◦ Aroma;
◦ Creative arts;
◦ Dance;
◦ Equine or other animal-assisted;
◦ Music;
◦ Play;
◦ Recreational or similar therapy; and
◦ Sensory movement groups.
2. Air ambulance, if ground ambulance would serve the same purpose
3. Ambulance (all types), to move you to a facility closer to your home or for purposes that are not
medically necessary
4. Autologous blood and platelet-rich plasma injections
5. Bariatric surgery under the following circumstances:
◦ BMI 30 to less than 35 without Type II Diabetes Mellitus
◦ BMI less than 30
◦ Patients younger than 18 years of age
6. Bone growth stimulators for:
◦ Nonunion of skull, vertebrae, or tumor related
2024 UMP CDHP (PEBB) Certificate of Coverage 107
◦ Ultrasonic stimulator – delayed fractures and concurrent use with another noninvasive stimulator.
7. Bone morphogenetic protein-7 (rhBMP-7) for use in lumbar fusion
8. Bronchial thermoplasty for asthma
9. Carotid artery stenting of intracranial arteries
10. Carotid intima media thickness testing
11. Catheter ablation for non-reentrant supraventricular tachycardia
12. Cervical spinal fusion without evidence of radiculopathy or myelopathy
13. Complications arising directly from services that would not be covered by the plan during the
current plan year. The plan will cover complications arising directly from services that a PEBB plan
covered for you in the past.
14. Computed Tomographic Colonography (CTC), also called a virtual colonoscopy, for routine
colorectal cancer screening
15. Corneal Refractive Therapy (CRT), also called Orthokeratology
16. Coronary or cardiac artery calcium scoring
17. Cosmetic services or supplies, including drugs and pharmaceuticals, unless part of the following
care:
◦ Reconstructive breast surgery following a mastectomy necessitated by disease, illness, or injury
◦ Reconstructive surgery of a congenital anomaly, such as cleft lip or palate, to improve or restore
function
18. Court-ordered care, unless determined by the plan to be medically necessary and otherwise covered
19. Custodial care (see definition on page 172)
20. Deep brain stimulation and transcranial direct current stimulation when used as nonpharmacological
treatments for treatment-resistant depression
21. Dental care for the treatment of problems with teeth or gums, other than the specific covered dental
services (see pages 45–46)
22. Dietary/food supplements, including, but not limited to:
◦ Herbal supplements, dietary supplements, and homeopathic drugs
◦ Infant or adult dietary formulas
◦ Medical foods (except when prescribed for inborn errors of metabolism)
◦ Minerals
◦ Prescription or over-the-counter vitamins (see page 91)
23. Dietary programs
24. Discography for patients with chronic low back pain and lumbar degenerative disc disease. This does
not apply to patients with the following conditions:
◦ Degenerative disease associated with significant deformity
◦ Fracture, tumor, infection, and inflammatory disease
◦ Functional neurologic deficits (motor weakness or Electromyography [EMG] findings of
radiculopathy)
108 2024 UMP CDHP (PEBB) Certificate of Coverage
◦ Isthmic spondylolysis
◦ Primary neurogenic claudication associated with stenosis
◦ Radiculopathy
◦ Spondylolisthesis greater than Grade 1
25. Drugs or medicines not covered by the plan, as described in the “Your prescription drug benefit”
section, see pages 87–103
26. Drugs or medicines obtained through mail-order pharmacies located outside the U.S.
27. Educational programs, except as described under:
◦ “Diabetes Control Program” on page 47
◦ “Diabetes education” on page 47
◦ “Diabetes Prevention Program” on page 47
◦ “Tobacco cessation services” on page 75
28. Electrical Neural Stimulation (ENS), which includes Transcutaneous Electrical Nerve Stimulation
(TENS) units, outside of medically supervised facility settings (e.g., in-home use).
29. Email consultations or e-visits, except as described under the telemedicine benefit.
30. Equipment not primarily intended to improve a medical condition or injury, including, but not
limited to:
◦ Air conditioners or air purifying systems
◦ Arch supports
◦ Communication aids
◦ Elevators
◦ Exercise equipment
◦ Massage devices
◦ Overbed tables
◦ Residential accessibility modifications
◦ Sanitary supplies
◦ Telephone alert systems
◦ Vision aids except when covered
through VSP
◦ Whirlpools, portable whirlpool pumps,
or sauna baths
31. Erectile or sexual dysfunction treatment with drugs or pharmaceuticals
32. Experimental or investigational services, supplies, or drugs (see page 174)
33. Extracorporeal shock wave therapy for musculoskeletal conditions
34. Eye surgery to alter the refractive character of the cornea, such as radial keratotomy,
photokeratectomy, or LASIK surgery
35. Facet neurotomy for headache
36. Facet neurotomy for thoracic spine
37. Fecal microbiota transplantation for treatment of inflammatory bowel disease
38. Foot care not related to diabetes: Toenail cutting; diagnosed corns and calluses treatment; or any
other maintenance-related foot care
39. Functional neuroimaging for primary degenerative dementia or mild cognitive impairment
40. Gene expression profile testing for multiple myeloma or colon cancer
41. Headaches:
2024 UMP CDHP (PEBB) Certificate of Coverage 109
◦ Treatment of chronic tension-type headache with Botox or acupuncture
◦ Treatment of chronic migraine or chronic tension-type headache with massage, trigger point
injections, transcranial magnetic stimulation, or manipulation/manual therapy (e.g., chiropractic
services).
Note: For chronic migraines and tension-type headaches, see page 53
42. Hearing aid items:
◦ Over-the-counter hearing aids that are not prescribed, except for initial assessment, fitting,
adjustment, auditory training, and ear molds as necessary to maintain an optimal fit
◦ Charges incurred after your plan coverage ends, unless you ordered the hearing aid before that
date and it is delivered within 45 days after your coverage ended
◦ Extended warranties, or warranties not related to the initial purchase of the hearing aid(s)
◦ Purchase of replacement batteries or other ancillary equipment, except those covered under
terms of the initial hearing aid purchase
The types of ancillary equipment not covered are:
◦ Alerting devices
◦ Assistive listening devices for FM/DM systems, receivers and transmitters
◦ Assistive listening devices for microphone transmitters
◦ Assistive listening devices for TDD machines
◦ Assistive listening devices for telephones
◦ Assistive listening devices for televisions (including amplifiers and caption decoders)
◦ Assistive listening devices for use with cochlear implants
◦ Assistive listening devices, supplies, and accessories not otherwise specified
43. Hip resurfacing
44. Hip surgery for treatment of Femoroacetabular Impingement (FAI) Syndrome
45. Home health care, except as described on page 54. The plan does not cover the following services:
◦ Housekeeping or meal services
◦ Care in any nursing home or convalescent facility
◦ Care provided by a family member
46. Hospital inpatient charges for non-essential services or features, such as:
◦ Admissions solely for diagnostic procedures that could be performed on an outpatient basis
◦ Personal or convenience items
◦ Reserved beds
◦ Services and devices that are not medically necessary (see definition on page 180)
47. Hyperbaric oxygen therapy treatment for:
◦ Acute and chronic sensorineural hearing loss
◦ Brain injury including traumatic (TBI) and chronic brain injury
110 2024 UMP CDHP (PEBB) Certificate of Coverage
◦ Cerebral palsy
◦ Migraine or cluster headaches
◦ Multiple sclerosis
◦ Non-healing venous, arterial, and pressure ulcers
◦ Thermal burns
48. Imaging of the sinus for rhinosinusitis using x-ray or ultrasound
49. Immunizations, physical exams and associated services (laboratory or similar tests) for the purpose
of travel or employment, even if recommended by the CDC
50. Implantable drug delivery systems (IDDS or infusion pumps) for chronic, non-cancer pain
51. Incarceration: Services and supplies provided while confined in a prison or jail
52. Infertility or fertility testing or treatment after initial diagnosis, including drugs, pharmaceuticals,
artificial insemination, and any other type of testing, treatment, complications resulting from such
treatment (e.g., selective fetal reduction), or visits for infertility
53. In Vitro Fertilization (IVF) and all related services and supplies, including all procedures involving
selection of embryo for implantation
54. Knee arthroplasty: Multi-compartmental arthroplasty and partial knee arthroplasty (including bi-
compartmental and bi-unicompartmental)
55. Knee arthroscopy for osteoarthritis of the knee
56. Late fees, finance charges, or collections charges
57. Learning disabilities treatment after diagnosis, except as covered under the following benefits:
◦ “Applied Behavior Analysis (ABA) Therapy” on page 40;
◦ “Therapy: Habilitative and Rehabilitative” on page 74;
◦ When part of treating a mental health disorder; or
◦ When part of treating a substance use disorder.
58. INTENTIONALLY LEFT BLANK.
59. Lumbar artificial disc replacement
60. Lumbar fusion for degenerative disc disease
61. Lumbar radiculopathy/sciatica surgery: Minimally invasive procedures that do not include
laminectomy, laminotomy, or foraminotomy, including, but not limited to, energy ablation
techniques, Automated Percutaneous Lumbar Discectomy (APLD), percutaneous laser, nucleoplasty,
etc.
62. Magnetic resonance imaging, (upright) (uMRI), also known as “positional,” “weight-bearing” (partial
or full), or “axial loading”
63. Maintenance care (see definition on page 179)
64. Manipulations of the spine or extremities, except as described under “Spinal and extremity
manipulations” on page 70
65. Marriage, family, or other counseling or training services, except as provided to treat an individual
member’s neuropsychiatric, mental health, or substance use disorder
66. Massage therapy services when the massage therapist is not a preferred provider
2024 UMP CDHP (PEBB) Certificate of Coverage 111
67. Medicare-covered services or supplies delivered by a provider who does not offer services through
Medicare, when Medicare is the member’s primary coverage
68. Microprocessor-controlled lower limb prostheses (MCP) for the feet and ankle
69. Migraine and tension-type headaches:
◦ Treatment of chronic tension-type headache with Botox or acupuncture
◦ Treatment of chronic migraine or chronic tension-type headache with massage, trigger point
injections, transcranial magnetic stimulation, or manipulation/manual therapy (e.g., chiropractic
services)
Note: For chronic migraines and tension-type headaches, see page 53
70. Missed appointment charges
71. Negative pressure wound therapy in patients with contraindications referred to by the FDA Safety
Communication dated February 24, 2011
72. Noncovered provider types: Services delivered by providers not listed as a covered provider type
(see page 19)
73. Novocure (i.e., Optune) (tumor treating fields)
74. Orthoptic therapy except for the diagnosis of strabismus, a muscle disorder of the eye
75. Orthotics, foot or shoe: Items such as shoe inserts and other shoe modifications, except as specified
on page 50
76. Osteochondral allograft/autograft transplantation for joints other than the knee
77. Out-of-network provider charges that are above the allowed amount
78. Peripheral nerve ablation, using any technique, to treat limb pain for adults and children, including
for knee, hip, foot, or shoulder due to osteoarthritis or other conditions
79. Pharmacogenetic testing for patients being treated with oral anticoagulants
80. Pharmacogenomics testing for depression, mood disorders, psychosis, anxiety, attention deficit
hyperactivity disorder (ADHD), and substance use disorder
81. Positron Emission Tomography (PET) scans for routine surveillance of lymphoma
82. Prescription drug charges over the allowed amount, regardless of where purchased
83. Prescription drugs that require preauthorization, unless the request is:
◦ Approved by the plan
◦ Supported by medical justification from a clinician other than the member or the member’s family
84. Printing costs for medical records
85. Private duty nursing or continuous care in the member's home, except as described on pages 57 and
69
86. Proton beam therapy for individuals age 21 or older for conditions other than:
◦ Brain/spinal
◦ Esophageal
◦ Head/neck
◦ Hepatocellular carcinoma
◦ Ocular
◦ Skull-based
◦ Other primary cancers where all other
treatment options are contraindicated
112 2024 UMP CDHP (PEBB) Certificate of Coverage
after review by a multidisciplinary tumor
board
87. Provider administrative fees: Any charges for completing forms, copying records, or finance charges,
except for records requested by the plan to perform retrospective (i.e., post-payment) review
88. Repetitive transcranial magnetic stimulation for tinnitus
89. Replacement of lost, stolen, or damaged durable medical equipment (DME)
90. Replacement of prescription drugs that are any of the following:
◦ Confiscated or seized by Customs or
other authorities
◦ Contaminated
◦ Damaged
◦ Expired
◦ Lost or stolen
◦ Ruined
91. Residential treatment programs offered at facilities that do not meet the definition of Residential
Treatment Facility (see definition of “Residential treatment facility”)
92. Reversal of voluntary sterilization (vasectomy, tubal ligation, or similar procedures)
93. Riot, rebellion, and illegal acts: Services and supplies for treatment of an illness, injury, or condition
caused by a member’s voluntary participation in a riot, armed invasion or aggression, insurrection or
rebellion, or sustained by a member arising directly from an act deemed illegal by a court of law
94. Routine ultrasounds during pregnancy, except one in week 13 or earlier, one during weeks 13-28, or
high-risk pregnancies (see description on page 64)
95. Sacroiliac joint fusion: Minimally invasive and open sacroiliac joint fusion procedures in adults, age
18 or older, with chronic sacroiliac joint pain related to degenerative sacroiliitis and/or sacroiliac joint
disruption
96. Screening and monitoring tests for osteopenia/osteoporosis:
◦ Once treatment for osteoporosis has begun, serial monitoring is not covered
◦ Development of a fragility fracture alone is not a covered indication
97. Separate charges for records or reports
98. Service animals: Any expenses related to a service animal
99. Services covered by other insurance, including, but not limited to:
◦ Automobile no-fault
◦ Commercial premises
◦ General no-fault
◦ Homeowner’s
◦ Medical payments (Med-Pay)
◦ Motor vehicle
◦ Personal injury protection (PIP)
◦ Renter’s
◦ Underinsured or uninsured motorist
See page 132 for more about how this works.
100. Services delivered by providers or facilities delivering services outside the scope of their licenses
101. Services or supplies:
◦ For which no charge is made, or for which a charge would not have been made if you had no
health care coverage
2024 UMP CDHP (PEBB) Certificate of Coverage 113
◦ For which you are not obligated to pay
◦ Provided by a resident physician or intern acting in that capacity
◦ Provided by someone in the member’s family or household
◦ That are not medically necessary for the diagnosis and treatment of injury or illness or restoration
of physiological functions and are not covered as preventive care. This applies even if services are
prescribed, recommended, or approved by your provider.
◦ That are solely for comfort
102. Services performed during a noncovered service
103. Services performed primarily to ensure the success of a noncovered service, including, but not
limited to, a hiatal hernia repair done to ensure the success of a noncovered laparoscopic adjustable
gastric banding surgery
104. Services supplemental to digital mammography. When performed supplementary to digital
mammography for screening purposes for members with or without dense breasts, the following
procedures are not covered:
◦ Non-high-risk patients:
• Automated Breast Ultrasound (ABUS)
• Handheld Ultrasound (HHUS)
• Magnetic Resonance Imaging (MRI)
◦ High-risk patients:
• Automated breast ultrasound (ABUS)
• Handheld Ultrasound (HHUS)
• Magnetic Resonance Imaging (MRI) less than 11 months after a prior screening
105. Services, supplies, or drugs related to occupational injury or illness (see page 130)
106. Services, supplies, or items that require preauthorization unless the request is:
◦ Approved by the plan
◦ Supported by medical justification from a clinician other than the member or the family of a
member
107. Skilled nursing facility services or confinement:
◦ When primary use of the facility is as a place of residence
◦ When treatment is primarily custodial
108. Sleep apnea diagnosis and treatment as indicated in referenced Medicare national and local
coverage determinations
109. Sleep therapy services performed at the following locations are not covered:
◦ Emergency room services
◦ Inpatient hospitalization
◦ Urgent-care facilities
110. Sound therapies for treatment of tinnitus, including, but not limited to:
◦ Masking devices (sound maskers)
◦ Altered auditory stimuli
◦ Auditory attention training
114 2024 UMP CDHP (PEBB) Certificate of Coverage
111. Spinal cord stimulation for chronic neuropathic pain
112. Spinal injections, therapeutic (except as described under “Spinal injections” on page 70) of the
following types:
◦ Facet injections
◦ Intradiscal injections
◦ Medial branch nerve block injections
113. Spinal surgical procedures known as vertebroplasty, kyphoplasty, and sacroplasty
114. Stem cell therapies for musculoskeletal conditions
115. Stereotactic body radiation therapy for the treatment of primary tumor of the following cancer
types:
◦ Bone
◦ Head and neck
◦ Adrenal
◦ Melanoma
◦ Merkel cell
◦ Breast
◦ Ovarian
◦ Cervical
116. Stereotactic radiation surgery for conditions other than central nervous system primary and
metastatic tumors
117. Surrogacy
118. Telephone or virtual consultations or appointments, except as described under “Telemedicine
services” on page 77
119. Tinnitus specific therapies including, but not limited to:
◦ Tinnitus retraining therapy (TRT)
◦ Neuromonics tinnitus treatment (NTT)
◦ Tinnitus activities treatment (TAT)
◦ Tinnitus-masking counseling
120. Transcutaneous vagal nerve stimulation (does not include or apply to support of previous implanted
VNS)
121. Transcutaneous vagal nerve stimulation for epilepsy or depression
122. Travel, transportation, and lodging expenses, except as specified for ambulance services covered by
the plan (see page 39), or approved travel and lodging costs related to the COE Program for single
knee and single hip replacement (see page 58) and for spine care (see page 70)
123. Treatment of varicose veins with Endovenous Laser Ablation (EVLA), Radiofrequency Ablation (RFA),
Sclerotherapy, and Phlebectomy in patients with pregnancy, active infection, peripheral arterial
disease, or deep vein thrombosis (DVT)
2024 UMP CDHP (PEBB) Certificate of Coverage 115
124. Upright magnetic resonance imaging (uMRI), also known as “positional,” “weight-bearing” (partial or
full), or “axial loading”
125. Vagal nerve stimulation (VNS) for treatment-resistant depression
126. Vagal nerve stimulation (VNS) for the treatment of depression (does not include or apply to support
of previously implanted VNS)
127. Vision hardware replacements:
◦ The plan does not cover the replacement of any lost, stolen or broken lenses and/or frames.
128. Vision, routine:
◦ Certain contact lens expenses:
• Artistically-painted or nonprescription contact lenses;
• Contact lens modification, polishing or cleaning;
• Refitting of contact lenses after the initial (90-day) fitting period;
• Additional office visits associated with contact lens pathology; and
• Contact lens insurance policies or service agreements.
◦ Corrective vision treatment of an experimental or investigational nature
• The VSP benefits do not cover investigational or experimental treatments or procedures (health
interventions), services, supplies, and accommodations provided in connection with health
interventions.
◦ Lens enhancements: The VSP benefits do not cover lens enhancements, including, but not limited
to:
• Anti-reflective coating;
• Color coating;
• Mirror coating;
• Scratch-resistant coating;*
• Blended lenses;
• Cosmetic lenses;
• Laminated lenses;
• Oversize lenses;
• Premium and custom progressive multifocal lenses;
• Photochromic lenses;
• Tinted lenses, except Pink #1 and Pink #2;
• UV (ultraviolet) protected lenses;* and
• Impact-resistant coating.*
*These lens enhancements are covered for children under age 19. Impact-resistant coating is
also covered for dependent children age 19 or older.
◦ Medical or surgical treatment of the eyes
129. Vision services and supplies:
◦ The plan does not cover services or supplies that are not medically necessary:
• Plano lenses (less than a ± .50 diopter power).
• Two pair of glasses instead of bifocals.
• Services and/or materials not described as covered under this vision benefit.
130. Vitamin D screening and testing as part of routine screening
131. Weight control, weight loss, and obesity treatment:
◦ Non-surgical: Any program, drugs, services, or supplies for weight control, weight loss, or obesity
treatment. Exercise or diet programs (formal or informal), exercise equipment, or travel expenses

116 2024 UMP CDHP (PEBB) Certificate of Coverage
relating to non-surgical or surgical services are not covered. Such treatment is not covered even if
prescribed by a provider, except as covered under "Bariatric surgery" (see page 41), “Diabetes
Control Program” (see page 47), “Diabetes Prevention Program” (see page 47), “Nutrition
counseling and therapy” (see page 62), or “Preventive care” (see page 65).
◦ Surgical: Any bariatric surgery procedure, any other surgery for obesity or morbid obesity, and
any related medical services, drugs, or supplies, except when approved by preauthorization
review.
132. Whole exome sequencing for:
◦ Uncomplicated autism spectrum disorder, developmental delay, mild to moderate global
developmental delay.
◦ Other circumstances (e.g. environmental exposures, injury, infection) that reasonably explain the
constellation of symptoms.
◦ Carrier testing for “at risk” relatives.
◦ Prenatal or pre-implantation testing.
133. Workers’ compensation: When a claim for workers’ compensation is accepted, all services related to
that injury or illness are not covered, even if some services are denied by workers’ compensation
134. Transcranial Magnetic Stimulation (TMS) for treatment of:
◦ Obsessive-compulsive disorder (OCD)
◦ Generalized anxiety disorder (GAD)
◦ Posttraumatic stress disorder (PTSD)
◦ Smoking cessation
◦ Substance use disorder (SUD)
If you have questions about whether a certain service or supply is covered, contact UMP Customer
Service.
If you have other HDHP coverage
Coordination of benefits
Coordination of benefits (COB) happens when you have health coverage through two or more groups
(such as your employer and your spouse’s employer), and these two group health plans both pay a
portion of your health care claims.
The rules beginning under the “Who pays first” section determine which plan pays first (primary payer)
and which pays second (secondary payer). See page 119 for a description of how the plan coordinates
benefits when it pays second.
The plan processes claims differently depending on if it is the primary payer or the secondary payer. The
differences are described in the next several pages.
TIP: If you have other health coverage, it is important that you let your providers know,
including the pharmacies where you get your prescription drugs.
2024 UMP CDHP (PEBB) Certificate of Coverage 117
Contact UMP and WSRxS
If you or your dependents have other insurance, you must let UMP and WSRxS know so claims are
processed correctly. To do this, you must complete and submit a separate form for medical services and
prescription drugs. Each person claiming payment for benefits under the plan is required to give Regence
and WSRxS any facts needed to apply these COB rules.
If your coverage under other plans changes, you must let UMP and WSRxS know so claims are processed
correctly. See the Directory pages at the beginning of this booklet for contact information and ways to get
and submit COB forms.
Who pays first
Note: If you cannot determine which plan pays first, contact UMP Customer Service.
Alert: Medicare will be the primary payer for covered benefits provided to Medicare-eligible
members who are enrolled in UMP as a dependent of a currently employed state-registered
domestic partner. Medicare will remain the secondary payer for benefits payable under UMP
for (1) individuals age 65 or over who have UMP as a result of their own current employee
status, or (2) individuals age 65 or over who have UMP as a result of the current employment
status of a spouse of any age.
When UMP coordinates benefits with other plans, the following rules determine which plan pays first.
These rules apply in order, so the first rule below that applies to your situation will determine which plan
is your primary coverage, and subsequent rules will not apply.
The following plan pays first:
• Any group plan that does not coordinate benefits.
• The plan that covers the member as a subscriber, not a dependent.
Exception: When the subscriber is a Medicare beneficiary, the plan covering the person as the retiree is
secondary to the plan covering the person as a dependent.
• The plan that covers the member (or their spouse or state-registered domestic partner) as an active
employee pays before a plan that covers the member as a retired employee.
• A plan covering the member as an employee, subscriber, retiree, or the dependent of such an
employee, subscriber, or retiree will pay before a COBRA or a state right of continuation plan.
• If the other plan is Medicare, UMP pays first if the member is age 65 or over who have UMP as a result
of their own active employee status or the active employee status of a spouse of any age. Note:
Medicare benefits are primary to UMP for members who are enrolled in UMP as a dependent of a
currently employed state-registered domestic partner.
• The plan that has covered the member (or their spouse or state-registered domestic partner) as a
subscriber the longest, if there are two plans and the first five bullets do not determine which plan pays
first.
• If none of the preceding rules determines the order of benefits, the allowable expenses must be shared
equally between the plans.
118 2024 UMP CDHP (PEBB) Certificate of Coverage
For dependent children
A group plan is usually primary over Medicaid programs that cover children. If a dependent child has
group coverage through their employer, the child’s coverage pays first.
Dependent children of married parents
The group plan of the parent whose birthday is earlier in the year pays first. For example, the plan of a
parent born April 14 is primary over the plan of a parent born August 21. This is called the “birthday rule.”
This rule looks only at the month and day, not the year. If both parents have the same birthday, the plan
that has covered either parent the longest is primary.
Exception for newborn children
Under Washington State law, the plan must cover newborns under the mother’s coverage for the first 21
days of life. Therefore, the mother’s plan pays first for covered charges during the first 21 days of a
newborn’s life.
Dependent children of legally separated or divorced parents
When no court order specifies which parent is responsible for providing health insurance coverage, the
following standard COB rules determine which plan pays first:
1. The plan of the custodial parent.
2. The plan of the custodial parent’s spouse, if the custodial parent has remarried.
3. The plan of the non-custodial parent.
4. The plan of the non-custodial parent’s spouse, if the non-custodial parent has remarried.
The custodial parent is the parent awarded custody by a court decree or, in the absence of a court decree,
is the parent with whom the child resides more than one half of the calendar year, excluding any
temporary visitation.
The birthday rule is used to determine which parent’s plan pays first if:
• The court order states that both parents are responsible for the child’s/children’s health coverage and
expenses.
• The court order awards joint custody without specifying that one parent is responsible for the
child’s/children’s health coverage and expenses.
If the court order states one parent is to assume primary financial responsibility for the child but does not
specify that one parent is responsible for health coverage and health care expenses, the plan of the parent
assuming financial responsibility is the primary payer.
In some cases, a court order determines payment for health care expenses. In those cases, standard COB
rules may not apply. You must promptly provide the plan with copies of the court order for the plan to
determine which plan pays first.
If a dependent child is covered under more than one plan through persons who are not the child’s parent
or stepparent (e.g., a grandparent or other guardian), the plan will use the birthday rule to determine
which plan pays first.
If none of the preceding rules determine who pays first, then each plan covers half of the allowed
expenses.
Federal and military plans
UMP usually pays first over certain federal or military programs for veterans (retired military members).
2024 UMP CDHP (PEBB) Certificate of Coverage 119
When UMP pays first
When the plan is the primary payer (pays first), UMP pays its normal benefit as described in this COC. You
may need to send UMP’s Explanation of Benefits and a copy of your provider’s bill to your secondary
payer to receive payment. Check with that plan for more information.
When UMP is supposed to pay first, but another plan did instead
If another plan pays first on claims where UMP should have paid first:
• UMP may pay the other plan the amount UMP should have paid.
• Amounts UMP pays to the other plan are considered benefits paid by UMP.
How UMP coordinates benefits when it pays second
UMP uses a type of COB called nonduplication of benefits (see definition of “Nonduplication of benefits”).
When UMP pays second to another plan that covers the member, UMP will pay only an amount needed to
bring the total benefit up to the amount UMP would have paid if the member did not have another plan.
The intent of this type of COB is to maintain the level of benefits available through UMP. The
nonduplication of benefits type of coordination is not designed to pay your covered expenses in full.
When UMP pays second, it coordinates with these types of plans:
• Governmental programs including, but not limited to, Medicare and Medicaid.
• Group, blanket, or franchise health or disability insurance policies; health care service contractor and
health maintenance organization group agreements issued by insurers; health care service contractors;
and health maintenance organizations.
• Labor management trusteed plans, labor organization plans, employer plans, or employee benefit
organization plans.
ALERT! If you have other primary coverage that pays for services, those services will apply to
the UMP benefit limit.
How much you may pay when UMP pays second
When you see preferred providers under UMP, you will owe only the balance of the UMP allowed amount
after your primary plan and UMP pay benefits for covered services. Your cost will usually be higher if you
see out-of-network providers. See the “Sample payments to different provider network status” section for
examples.
The examples in the table below assume that you have met your deductible.
Situation
Example
Preferred
provider
charge
UMP
allowed
amount
UMP
normal
benefit
Other
plan
pays
UMP
pays
You pay
your
provider
UMP is
primary,
other plan
is
secondary
EXAMPLE 1:
When UMP
pays first (or
is the only
plan)
$200
$100
$85
(85% of
$100)
N/A
$85
$15
UMP is
secondary,
EXAMPLE 2:
$200
$100
$85
$80
$5
$15
120 2024 UMP CDHP (PEBB) Certificate of Coverage
Situation
Example
Preferred
provider
charge
UMP
allowed
amount
UMP
normal
benefit
Other
plan
pays
UMP
pays
You pay
your
provider
other plan
is primary
The other
plan pays
less than the
normal UMP
benefit
UMP is
secondary,
other plan
is primary
EXAMPLE 3:
The other
plan pays as
much as (or
more than)
the normal
UMP benefit
$200
$100
$85
$85
$0
$15
Contact UMP Customer Service for help with any questions if you are covered by more than one plan.
Submit secondary claims promptly
All health plans have a “timely submitting” deadline. The timely submitting deadline for UMP is 12 months
from the date of service. If a claim is not submitted within the plan’s timely submitting deadline, UMP will
deny it. If your primary plan delays payment on a claim, you must still submit to UMP within the
submitting deadline to prevent denial of the claim.
UMP may try to contact your primary plan for their benefit payment information or may estimate it to
provide timely processing of your secondary benefit. Adjustments may be made when the primary plan
pays their portion of your claim. Notifying your providers of any change to your coverage will help avoid
errors and delays in processing of claims (see the “Billing and payment: submitting a claim” section).
How diabetes care supplies are covered when UMP pays second
UMP covers diabetes care supplies under the prescription drug benefit. If you get your supplies from a
pharmacy, ask if the pharmacy can bill both your primary plan and UMP. If your pharmacy does, you do
not need to do anything further. If not, you will need to send a claim to WSRxS for secondary payment
(see the “Submitting a claim for prescription drugs” section for instructions).
If you get your supplies from a diabetes care supplier, the primary plan may process the claim as medical.
In this case, you need to send your Explanation of Benefits and a claim form to WSRxS for secondary
payment (see the “Submitting a claim for prescription drugs” and the “False claims or statements” sections
for instructions).
Note: Nonduplication of benefits applies to these claims, which means that UMP may pay nothing after
your primary plan pays.
See the “Diabetes care supplies” benefit for more information.
ALERT! You must submit secondary claims for diabetes care supplies to WSRxS. Regence
BlueShield will deny these claims.

2024 UMP CDHP (PEBB) Certificate of Coverage 121
How COB works with prescription drugs
Some of the limits and restrictions to prescription drug coverage listed in the “Limits on your prescription
drug coverage” section will apply when UMP pays second to another plan. See the “Submitting a claim for
prescription drugs” section for how to submit your prescription drug claim.
Nonduplication of benefits applies when UMP pays second to another plan. This means that UMP may
pay nothing after your primary plan pays.
Using network pharmacies when UMP is secondary
If you have primary coverage through another plan that covers prescription drugs, show both plan
member ID cards to the pharmacy and make sure they know which plan pays first and which plan pays
second. It is important that the pharmacy bills the plans in the correct order, or claims may be denied or
paid incorrectly.
Using mail-order pharmacies when UMP is secondary
If your primary plan also uses one of UMP’s network mail-order pharmacies as the plan’s network mail-
order pharmacy, UMP’s network mail-order pharmacies may process payments for both plans and charge
you only the remainder. Make sure that UMP’s network mail-order pharmacies have the information for
both plans and know which plan is primary.
However, if your primary plan uses a different mail-order pharmacy, you will have to use your primary
plan’s mail-order pharmacy, then submit a paper claim to UMP. See the “Submitting a claim for
prescription drugs” section for how to do this.
Billing and payment: submitting a claim
Submitting a claim for medical services
When UMP is your primary insurance and your provider is preferred, or participating, you do not need to
submit claims. The provider will do it for you. If you have a question about whether your provider’s office
has submitted a claim, sign in to your Regence account or contact UMP Customer Service (see Directory
for link and contact information). See the “Submitting a Blue Cross Blue Shield Global® Core claim”
section on page 24 for instructions on submitting a claim for services received outside of the United
States.
TIP: In the following section, Uniform Medical Plan (UMP) refers to the administrative functions
for submitting claims to UMP. Regence BlueShield handles medical claims, and WSRxS handles
prescription drugs claims.
When you need to submit a claim
You may need to submit a claim to UMP for payment if:
• You receive services from an out-of-network provider.
• You have other insurance that pays first and UMP is secondary.
Out-of-network providers may submit a claim on your behalf. Ask your provider.

122 2024 UMP CDHP (PEBB) Certificate of Coverage
How to submit a claim
To submit a claim yourself, you may sign in to your Regence account and go to the Submit claim
webpage at regence.com/member/submit-claim/ or you may complete a medical claim form and mail
the following documents:
• UMP (Regence) Medical Claim Form — You may find the form by visiting forms and publications at
hca.wa.gov/ump-forms-pubs or you may request a form by contacting UMP Customer Service.
• An itemized bill from your provider that describes the services you received and the charges.
The following information must appear on the provider’s itemized bill for the plan to consider the claim
for payment:
• Member’s name and member ID number, including the alpha prefix (three letters and the ‘W’ before
member ID number)
• Procedure and diagnosis code(s) or description of the injury or illness
• Date and type of service
• Provider’s name, address, phone number, and National Provider Identifier (NPI) or Tax ID number
• For ambulance claims, also include the ZIP code of where the member was picked up and where they
were taken
If UMP is secondary, you must include a copy of your primary plan’s Explanation of Benefits, which lists
the services covered and how much the other plan paid. You should wait until the primary plan has paid
to submit a secondary claim to UMP, unless the primary plan’s processing of the claim is delayed. Claims
not submitted to UMP within 12 months of the date of service will not be paid.
If we must request additional information, the processing of your claim may be delayed.
Note: Be sure to make copies of your documents for your records.
Mail both the claim form and the provider’s claim document (or bill) to:
Regence BlueShield
Attn: UMP Claims
PO Box 1106
Lewiston, ID 83501-1106
Or you can fax documents to Regence at 1-877-357-3418.
The plan may send reimbursement for services received from an out-of-network provider to the provider
or to you in the form of a check listing both you and the provider as payees. If you paid up front for
services, proof of payment may be required. Contact UMP Customer Service if you have a question about
the processing of your claim or for information on what is acceptable as proof of payment.
Important information about submitting claims
ALERT! You or your provider must submit claims within 12 months of the date you received
health care services. This is called the “timely submitting” deadline. The plan will not pay claims
submitted more than 12 months after the date of service. See “Submit secondary claims
promptly” on page 120 for how this works when you have other coverage that pays first.

2024 UMP CDHP (PEBB) Certificate of Coverage 123
For information about submitting claims for services outside of the U.S., contact UMP Customer Service.
You may have to pay services upfront and submit a claim for reimbursement.
If you have other health care coverage, see the “If you have other HDHP coverage” section for information
on how the plan coordinates benefits with other plans.
Services apply to your UMP deductible in the order claims are received, not necessarily in the order the
member receives services.
Claims reimbursement
Most of the time, the plan will pay preferred or participating providers directly. For claims submitted by
you or an out-of-network provider, the plan will determine whether to pay you, the provider, or both. For
a child covered by a legal qualified medical child support order (see page 118) the plan may pay the
child’s custodial parent or legal guardian.
Claims determinations
The plan will notify you of action taken on a claim within 30 days of the plan receiving it. This 30-day
period may be extended by 15 days when action cannot be taken on the claim due to:
• Circumstances beyond the plan’s control. Notice will include an explanation why an extension is
needed and when the plan expects to act on the claim.
• Lack of information. The plan will notify you within the 30-day period that an extension is necessary,
with a description of the information needed and why it is needed.
Submitting a claim for prescription drugs
You may need to submit your own prescription drug claim to WSRxS for reimbursement if you:
• Buy prescription drugs at a non-network retail pharmacy.
• Fail to show your UMP member ID card at a network pharmacy.
• Have other prescription coverage that pays first, and UMP is secondary.
TIP: If you get a vaccine from an out-of-network provider, make sure that you submit your
claim to Regence BlueShield as a medical claim (see the “Submitting a claim for medical
services” section).
Prescription drug claim forms are available by visiting forms and publications at hca.wa.gov/ump-forms-
pubs or by contacting WSRxS Customer Service. Send the completed claim form, along with your
pharmacy receipt(s), to:
Pharmacy Manual Claims
PO Box 999
Appleton, WI 54912-0999
It is a good idea to keep copies of all your paperwork for your records.
When you submit a prescription drug claim to WSRxS, the plan pays the claim based on the following
rules, no matter where you purchased the drug:
• The plan pays based on the allowed amount. If the pharmacy charges you more than the allowed
amount, you will pay your usual coinsurance (and deductible if applicable), plus the difference between
what the plan paid and the pharmacy’s charge.
124 2024 UMP CDHP (PEBB) Certificate of Coverage
• The plan pays all prescription drug claims, including non-network retail pharmacies, based on
coinsurance.
• If your claim exceeds the quantity limit or the maximum days’ supply allowed by the plan, the plan will
pay only for the amount of the prescription drug up to the quantity limit or maximum days’ supply.
• If you receive a refill before 84 percent of the last supply you received should have been taken, the plan
will not pay for it. (see the “Refill too soon” section).
You must submit prescription drug claims within 12 months of purchase. The plan will not pay claims for
prescription drugs submitted more than 12 months after purchase or prescription drugs purchased from
an excluded pharmacy. See the definition of “Excluded pharmacy.”
ALERT! If you do not show your UMP member ID card when purchasing a prescription at a
network pharmacy, you will have to pay the full cash price and submit a Prescription Drug
Claim Form. You will not receive the plan discount.
False claims or statements
Neither you nor your provider (or any person acting for you or your provider) may submit a claim for
services or supplies that were not received, were resold to another party, or for which you are not
expected to pay.
In addition, neither you nor any person acting for you may make any false or incomplete statements or
any false claims on any document for your plan coverage.
The plan may recover any payments or overpayments made because of a false claim or false statement by
withholding future claim payments, by suing you, or by other means. False claims may also be crimes.
If you represent yourself as being enrolled in this plan when you are not, the plan will deny all claims.
If the plan asks you for more information, you will be allowed at least 45 days to provide it. If the plan
does not receive the information requested within the time allowed, the plan will deny the claim.
Complaint and appeal procedures
ALERT! In the following section, UMP refers to the administrative functions for appeals for
UMP CDHP. Regence BlueShield handles medical appeals; WSRxS handles appeals involving
prescription drugs; and Premera handles appeals for the COE Program. See the “Joint
replacement surgery, knees and hips in the Centers of Excellence (COE) Program” and “Spine
care in the Centers of Excellence (COE) Program” benefits for more information. VSP handles
appeals for routine vision benefits. See “Your routine vision benefits” for more information.
Appeals procedures may change during the year if required by federal or Washington State
law.
What is a complaint (aka: grievance)?
A complaint is an oral statement or written document submitted by or on behalf of a member regarding:

2024 UMP CDHP (PEBB) Certificate of Coverage 125
• Dissatisfaction with medical care.
• Dissatisfaction with service provided by the health plan.
• Provider or staff attitude or demeanor.
• Waiting time for medical services.
Note: If your issue is regarding a denial, reduction, or termination of payment or nonprovision of medical
services, it is an appeal.
How to submit a complaint (aka: grievance)
For all medical complaints, it’s recommended that you first contact UMP Customer Service. For
prescription drug complaints or grievances, we recommend contacting WSRxS Customer Service. Many
issues may be resolved with a phone call. If an initial phone call does not resolve your complaint, you may
submit your complaint:
• Over the phone: If you want a written response, you must request one.
• By mail, fax, or email (see the “Where to send complaints or appeals” section below).
You will receive notice of the action on your complaint or grievance within 30 calendar days of our
receiving it. The plan will notify you if it needs more time to respond.
What is an appeal?
An appeal is an oral or written request submitted by you or your authorized representative to Regence
BlueShield or WSRxS to reconsider:
• A decision to deny, modify, reduce, or terminate payment, coverage, certification, or provision of health
care services or benefits, including the admission to, or continued stay in, a health care facility.
• A preauthorization.
• A retroactive decision to deny coverage based on eligibility (see the “Appeals related to eligibility”
section below).
• Claims payment, processing, or reimbursement for health care services or supplies.
The appeals process
ALERT! If your appeal is for an urgent or life-threatening condition, see the "Expedited appeals
process" section below.
You or someone you authorize to represent you (see “How to designate an authorized representative” on
page 136) may submit an appeal. There are three levels to the appeals process:
1. First-level appeal
2. Second-level appeal
3. External review (independent review)
Each of those parts are described in further detail below.
126 2024 UMP CDHP (PEBB) Certificate of Coverage
Coverage during each review
If your request involves a decision to change, reduce, or terminate coverage for services, supplies, or
prescription drugs already being covered, the plan must continue to cover the disputed service until the
outcome of the review. If the plan upholds the decision to change, reduce, or terminate coverage, you will
be responsible for the cost of the services received during the review period. If you request payment for
denied claims or approval of services, supplies, or prescription drugs not yet covered by the plan, the plan
will not cover the services, supplies, or prescription drugs while the appeal is under consideration.
First-level and second-level appeal reviewers
Claim processing disputes will be reviewed by administrative staff. The plan will consult with a health care
professional employed by Regence BlueShield on medical appeals, or with a health care professional
employed by Washington State Rx Services on prescription drug appeals, when appeals involve issues
requiring medical judgment about covering, authorizing, or providing health care. That includes decisions
based on determinations that a treatment, prescription drug, or other item is experimental,
investigational, or not medically necessary. Your appeal will be reviewed by Regence BlueShield or
Washington State Rx Services employees who have not been involved in, or subordinate to anyone
involved in, reviewing the previous decisions.
How to submit an appeal
You or your authorized representative (including a relative, friend, advocate, attorney, or provider) may
submit an appeal by using the methods described below in the “Where to send complaints or appeals”
section. You may authorize a representative to submit an appeal on your behalf in writing or by
contacting UMP Customer Service (medical appeals) or WSRxS Customer Service (prescription drug
appeals).
For each appeal request, you must appeal within 180 days of receiving the plan’s decision. You may
include written comments, documents, and any other information, such as medical records and letters
from your provider, to support your appeal request. The plan will consider all information submitted when
reviewing your appeal. You may also request copies of documents the plan has that are relevant to your
appeal, which the plan will provide at no cost to you.
The plan will mail you a written response within 14 days of receiving your appeal request. If more time is
needed to thoroughly research and review your appeal, the plan is allowed up to 30 days to respond. The
plan will ask your permission if it needs more time to respond. You can access the UMP (Regence) Medical
appeals and grievance form by visiting forms and publications at hca.wa.gov/ump-forms-pubs.
Information to provide with an appeal
You can submit information, documents, written comments, records, evidence, and testimony, including
second opinions, with your appeal. When you provide all the necessary documentation, it allows the plan
to review your appeal faster. Include the following when requesting an appeal:
• The member’s full name (the name of the employee, retiree, or dependent covered by the plan)
• The member ID number (starting with a “W” on your UMP member ID card)
• The name(s) of any providers involved in the issue you are appealing
• Date(s) of service or incident
• Your mailing address
• Your daytime phone number(s)
• A statement describing the issue and your desired outcome
• A copy of the Explanation of Benefits, if applicable, or a list of the claim numbers you are appealing

2024 UMP CDHP (PEBB) Certificate of Coverage 127
• Medical records from your provider, if applicable. Your provider should supply clinically relevant
information, such as medical records for services denied based on medical necessity or for other clinical
reasons. The plan must receive all relevant information with the appeal to make sure the most accurate
decision is made.
First-level appeals
You or your authorized representative may submit a first-level appeal no more than 180 days after you
receive the plan’s decision. If you do not submit an appeal within this time, your appeal will not be
reviewed, and you will not be able to continue further appeals (second-level and external review). You
may authorize a representative to submit an appeal on your behalf in writing or by contacting UMP
Customer Service (medical appeals) or WSRxS Customer Service (prescription drug appeals).
Regence BlueShield manages first-level appeals for medical services, and WSRxS manages first-level
appeals for prescription drugs. Employees from Regence BlueShield and WSRxS reviewing the appeals will
not have been involved in the initial decision you are appealing. Administrative staff review claim
processing disputes. A staff of health care professionals at Regence BlueShield or WSRxS evaluate appeals
that involve issues requiring medical judgment about covering, authorizing, or providing health care.
ALERT! Deadlines for submitting an appeal are based on the first date you are notified of how
a claim was processed, usually when you receive you an Explanation of Benefits (including
services that applied to your deductible or were denied). The plan does not waive deadlines
based on untimely billing by your provider.
Second-level appeals
If you disagree with the decision made on your first-level appeal, you or your authorized representative
may submit a second-level appeal. You must submit second-level appeals no more than 180 days after
you receive the letter responding to your first-level appeal. If you do not submit an appeal within this
time, your appeal will not be reviewed, and you will not be able to continue further appeals (external
review). You may authorize a representative to submit an appeal on your behalf in writing or by
contacting UMP Customer Service (medical appeals) or WSRxS Customer Service (prescription drug
appeals).
Regence BlueShield manages second-level appeals for medical services, and WSRxS manages second-
level appeals for prescription drugs. Employees from Regence BlueShield and WSRxS reviewing the
appeals will not have been involved in, or subordinate to anyone involved in, reviewing the first-level
appeal or initial decision. If new or additional evidence or rationale is considered in reviewing your appeal,
the plan will provide you with this information free of charge, and you may respond before the final
decision.
Expedited appeals process
Expedited appeals for medical services
You or your authorized representative may submit an expedited appeal within 180 days of receiving the
previous decision if:
• You are currently receiving or prescribed treatment or benefits that would end because of the denial; or
• Your provider determines that taking the usual time allowed could seriously affect your life, health, or
ability to regain maximum function, or would subject you to severe pain that cannot be adequately
managed without the disputed care or treatment; or

128 2024 UMP CDHP (PEBB) Certificate of Coverage
• The issue is related to admission, availability of care, continued stay, or emergency health care services
and you have not been discharged from the emergency room or transport service.
You may authorize a representative to submit an expedited appeal on your behalf in writing or by
contacting UMP Customer Service.
An expedited appeal replaces both the first- and second-level appeals. Regence BlueShield will call you, or
your authorized representative, with a decision on your expedited appeal within 72 hours of the request.
Regence BlueShield will also mail a written response within 72 hours of the decision.
Your provider must submit all clinically relevant information to the plan by phone or fax at:
• Phone: 1-888-849-3682 (TRS: 711)
• Fax: 1-877-663-7526
If you disagree with the expedited appeal decision, your provider may request an expedited external
review (see the “External review (independent review)” section below).
Expedited appeals for prescription drugs
You or your authorized representative may submit an expedited appeal within 180 days of receiving the
previous decision if you or your provider thinks you need a prescription drug immediately. You may
authorize a representative to submit an appeal on your behalf in writing or by contacting WSRxS
Customer Service.
An expedited appeal replaces both the first- and second-level appeals. WSRxS will call you, or your
authorized representative, with a decision on your expedited appeal within 72 hours of the request.
WSRxS will also mail a written response within 72 hours of the decision.
You or your provider must submit all clinically relevant information to the plan by phone or fax at:
• Phone: 1-888-361-1611 (TRS: 711)
• Fax: 1-866-923-0412
During an expedited appeal, you may choose to purchase a three-day supply at your own expense. If
WSRxS decides to cover the prescription drug, WSRxS will reimburse you up to the allowed amount minus
the member cost-share (coinsurance and deductible, if applicable). If WSRxS decides not to cover the
prescription drug (denies the appeal), you are responsible for the full cost of the drug.
If you disagree with the expedited appeal decision, you or your provider may request an expedited
external review (see the “External review (independent review)” section below).
Time limits for the plan to decide appeals
ALERT! The plan will comply with shorter time limits than those below when required by
federal or Washington State law.
The time limits for both first- and second-level appeals are calculated from when the plan receives the
appeal. The plan will decide your appeal within 14 days of receiving it but may take up to 30 days unless a
different time limit applies as explained below. The plan will request written permission from you or your
authorized representative if an extension to the 30-day time limit is needed to get medical records or a
second opinion.
2024 UMP CDHP (PEBB) Certificate of Coverage 129
For expedited appeals, the plan will decide as soon as possible but always within 72 hours. The plan will
notify you (or your authorized representative) of the decision verbally within 72 hours and will mail a
written notice within 72 hours of the decision.
External review (independent review)
You or your authorized representative may submit a request for an external review by an independent
review organization (IRO) if you have gone through both a first- and second-level appeal (or expedited
appeal) and your appeal was based on the plan’s decision to deny, modify, reduce, or terminate coverage
of or payment for a health care service.
You may also submit a request for an external review:
• If the plan has exceeded the timelines for response to your appeal without good cause and without
reaching a decision; or
• If the plan has failed to adhere to the requirements of the appeals process.
You may submit a request for an expedited external review if you meet the requirements for the
expedited process as described above. You may also request an expedited external review at the same
time that you request an expedited appeal, called concurrent expedited review. When you request
concurrent expedited review, you are not required to go through both a first- and second-level appeal.
An IRO will conduct the external review. An IRO is a group of medical and benefit experts certified by the
Washington State Office of the Insurance Commissioner and not related to the plan, Regence BlueShield,
WSRxS, or HCA. An external review provides unbiased, independent clinical and benefit expertise to
determine whether the plan’s decision is consistent with state law and the 2024 UMP CDHP (PEBB)
Certificate of Coverage.
Requesting an external review
To request an external review, see the contact information listed in the “Where to send complaints or
appeals” section below.
You or your authorized representative must submit a request for an external review no more than 180
days after you receive the letter responding to your second-level appeal (or expedited appeal). Only the
member or an authorized representative may submit a request for an external review. You may authorize
a representative to submit a request for an external review on your behalf in writing or by contacting UMP
Customer Service (medical appeals) or WSRxS Customer Service (prescription drug appeals).
The plan — Regence BlueShield for medical services, and WSRxS for prescription drugs — will send the
IRO all of the relevant information and correspondence they considered in making the decision. You may
send more information directly to the IRO. The IRO will notify you of their decision.
Additional legal options
You are required to exhaust the plan’s appeals process before you may bring a cause of action in court
against the plan or HCA. If an IRO reviews your appeal, their decision is binding on both the plan and you
except to the extent that other remedies are available under state or federal law.
If the IRO overturns the plan’s decision the plan will provide benefits (including making payment on the
claim) according to the IRO’s decision without delay, regardless of whether the plan intends to seek
judicial review of the IRO’s decision and unless and until there is a judicial decision otherwise.
Complaints about quality of care
For complaints or concerns about the quality of care you received from preferred and participating
providers only, contact UMP Customer Service or send a secure email through your Regence account. See
Directory for link and contact information.

130 2024 UMP CDHP (PEBB) Certificate of Coverage
For complaints or concerns about the quality of care you received from any provider:
• Call Washington State Department of Health at 360-236-4700 (TRS: 711) or 1-800-562-6900 (TRS: 711).
• Email the Department of Health at HSQAComplaintIntake@doh.wa.gov.
• Visit the Department of Health website at doh.wa.gov/about-us/file-complaint.
Appeals related to eligibility
Appeals related to eligibility and enrollment are handled by the PEBB Program and governed by chapter
182-16 WAC.
Information on how to file an appeal is available:
• On the HCA website at hca.wa.gov/pebb-appeals.
• By contacting the PEBB Appeals Unit at 1-800-351-6827 (TRS: 711).
Where to send complaints or appeals
ALERT! Premera handles appeals for the COE Program. See the “Joint replacement surgery,
knees and hips in the Centers of Excellence (COE) Program” and “Spine care in the Centers of
Excellence (COE) Program” benefits for more information. VSP handles appeals for routine
vision benefits. See “Your routine vision benefits” for more information.
It is recommended that you call first with a complaint or appeal, since many problems may be resolved
quickly over the phone. The Directory at the beginning of this booklet includes links and contact
information to contact UMP (medical services) or WSRxS (prescription drugs) with a complaint or appeal.
When another party is responsible for injury or
illness
You may receive a letter from the plan asking if your injury or illness was the result of an accident or
might be someone else’s responsibility. To make sure claims are paid in a timely manner, it is important
that you respond as directed in the letter, even if the answer is no. If you do not, the plan may deny
coverage. You may contact UMP Customer Service if you have questions.
Occupational injury or illness (workers’ compensation) claims
When a claim for occupational injury or illness (workers’ compensation) is accepted by your employer’s
workers' compensation carrier, UMP will not cover any services related to that injury or illness, even if the
compensation carrier denies some services. You must file a workers’ compensation claim with your
workers’ compensation carrier. If your claim for workers’ compensation is denied because it is determined
the injury or condition is not related to an occupational injury or illness, UMP will pay for covered services
under the terms of this COC.
Legal rights and responsibilities
Coverage under the plan is not provided for medical, dental, prescription, or vision expenses you incur for
treatment of an injury or illness if the costs associated with the injury or illness may be covered by another
first party insurance or may be recoverable from any of the following:

2024 UMP CDHP (PEBB) Certificate of Coverage 131
• A third party;
• Any other source, including no fault automobile medical payments (Med-Pay), no fault automobile
personal injury protection (PIP), homeowner’s no-fault coverage, commercial premises no-fault medical
coverage, and sports policies. This includes excess, underinsured, or uninsured motorist coverage, or
similar contract or insurance, when the contract or insurance is either issued to or makes benefits
available to you, whether or not you make a claim under such coverage; or
• Services or supplies for work-related injury or illness, even when the service or supply is not a covered
workers’ compensation benefit under the workers’ compensation plan.
ALERT! You must respond to any communication sent to you about other sources of benefits,
or the plan may deny claims.
However, after expiration or exhaustion of the above benefits, if you also have a potential right of
recovery for illnesses or injuries from a third party who may have legal responsibility or from any other
source, benefits may be provided or advanced by the plan pending the resolution of a claim to the right
of recovery subject to all of the following conditions:
• By accepting or claiming benefits, you agree that the plan is entitled to reimbursement of the full
amount of benefits paid out of any settlement or recovery from any source to the extent that the
settlement or recovery exceeds full compensation to you for the injury or illness that you sustained.
This includes any arbitration award, judgment, settlement, disputed claim settlement, underinsured or
uninsured motorist payment, or any other recovery related to the injury or illness for which benefits
under the plan have been provided or advanced.
• The plan may choose to recover expenses directly from the third party (or third party’s insurer)
responsible for your injury or illness. This is called subrogation. The plan is authorized, but not
obligated, to recover any expenses, to the extent that they were paid under the plan, directly from any
party liable to you, upon mailing of a written notice to the potential payer, to you, or to your
representative.
• The plan’s rights apply without regard to the source of payment for medical expenses, whether from
the proceeds of any settlement, arbitration award, or judgment, or other characterization of the
recovery by you or any third party or the recovery source. The plan is entitled to reimbursement from
the first dollar received from any recovery to the extent that the settlement or recovery exceeds full
compensation to you for the injury or illness that you sustained. This applies regardless of whether:
▪ The third party or third party’s insurer admits liability;
▪ The health care expenses are itemized or expressly excluded in the recovery; or
▪ The recovery includes any amount (in whole or in part) for services, supplies, or accommodations
covered under the plan.
• You may be required to sign and deliver all legal papers and take any other actions requested to secure
the plan’s rights (including an assignment of rights to pursue your claim if you fail to pursue your claim
of recovery from the third party or other source). If you are asked to sign a trust/reimbursement
agreement or other document to reimburse the plan from the proceeds of any recovery, you will be
required to do so as a condition to advancement of any benefits. If you or your agent or attorney fail to
comply during the course of the case, we may request refunds from the providers or offset future
benefits.
132 2024 UMP CDHP (PEBB) Certificate of Coverage
• You will not do anything to prejudice the plan’s rights and that you will cooperate fully with the plan,
including signing any documents within the required time and providing prompt notice of any
settlement or other recovery. You must notify the plan of any facts that may impact the right to
reimbursement or subrogation, including, but not necessarily limited to, the following:
▪ The filing of a lawsuit;
▪ The making of a claim against any third party;
▪ Scheduling of settlement negotiations with a minimum of 21 days advance notice of the date, time,
location and participants to be involved in any settlement conferences or mediations); or
▪ Intent of a third party to make payment of any kind to your benefit or on your behalf and that in any
manner relates to the injury or illness that gives rise to the plan’s right of reimbursement or
subrogation (notice is required a minimum of five business days before the settlement).
• You and your agent or attorney must agree to keep segregated in its own account any recovery or
payment of any kind to your benefit that in any manner relates to the injury or illness giving rise to the
plan’s right of reimbursement or subrogation, until the plan’s right is satisfied or released.
• In the event you or your agent or attorney fails to comply with any of these conditions, any such
benefits provided or advanced for any illness or injury may be recovered through legal action to the
extent that the settlement or recovery exceeds full compensation to you for the injury or illness that
you sustained.
• Any benefits provided or advanced under the plan are provided or advanced solely to assist you. By
paying such benefits, the plan is not waiving any right to reimbursement or subrogation.
Fees and expenses
You may incur attorney’s fees and costs in connection with obtaining a recovery. We may pay a
proportional share of such attorney’s fees and costs you incur at the time of any settlement or recovery to
otherwise reduce the amount of reimbursement paid to the plan to less than the full amount of benefits
paid by the plan.
Services covered by other insurance
The plan does not cover services that are covered by other insurance, including, but not limited to, no
fault automobile medical payments (Med-Pay), no fault automobile personal injury protection (PIP),
homeowner’s no-fault coverage, commercial premises no fault medical coverage, or sports policies,
including excess, underinsured or uninsured motorist coverage or similar contract or insurance. You are
responsible for any cost-sharing required under the other coverage as allowed by state law. Once you
have exhausted benefits (e.g., reached the maximum medical expenses amount of the other insurance
policy (-ies), or services are no longer injury-related), the plan will cover services according to this COC.
Motor vehicle coverage
If you are involved in a motor vehicle accident, whether as a driver, passenger, pedestrian, or other
capacity, you may have rights under multiple motor vehicle insurance no fault coverages and also against
a third party who may be responsible for the accident. In that case, this right of reimbursement and
subrogation provision still applies.
Future medical expenses
Benefits for otherwise covered services may be excluded as follows:
2024 UMP CDHP (PEBB) Certificate of Coverage 133
• When you have received a recovery from another source relating to an illness or injury for services for
which we normally would provide benefits. The amount of any exclusions under this provision,
however, will not exceed the amount of your recovery.
• Until the total amount excluded equals the third-party recovery.
General provisions
UMP is administered by Regence BlueShield and Washington State Rx Services under contract with HCA.
What you need to know: your rights and responsibilities
To make sure UMP offers access to the best possible medical care, we must work together with you and
your providers as partners. To achieve this goal, you must know your rights and responsibilities.
As a plan member, you have the right to:
• Ask your provider to submit secondary claims to Medicare, if applicable.
• Be informed by your providers about all appropriate or medically necessary treatment options for your
condition, regardless of cost or benefit coverage.
• Be treated with respect.
• Complain about or appeal plan services or decisions, or the care you receive.
• Get a second opinion about your provider’s care recommendations.
• Have a translator’s assistance, if required, when contacting the plan.
• Keep your medical records and personal information confidential as described in the UMP Notice of
Privacy Practices, available online on the HCA website at hca.wa.gov/ump-privacy.
• Make decisions with your providers about your health care.
• Make recommendations about member rights and responsibilities.
• On request, receive information from the plan about:
▪ How new technology is evaluated for inclusion as a covered service.
▪ How the plan reimburses providers.
▪ Preauthorization review requirements.
▪ Providers you select and their qualifications.
▪ Services and treatments that have completed HTCC review and how that affects coverage by UMP.
▪ Technologies and treatments currently under review by the HTCC.
▪ The plan and preferred providers.
▪ Your covered expenses, exclusions, reductions, and maximums or limits.
• Receive:
▪ A written explanation from the plan about any request to refund an overpayment.
▪ All covered services and supplies determined to be medically necessary as described in this COC,
subject to the maximums, limits, exclusions, deductible, and coinsurance.
▪ Courteous, prompt answers from the plan.
134 2024 UMP CDHP (PEBB) Certificate of Coverage
▪ Timely, proper medical care without discrimination of any kind — regardless of health status or
condition, sex, ethnicity, race, marital status, color, national origin, age, disability, or religion.
As a plan member, you have the responsibility to:
• Comply with requests for information by the date given.
• Confirm provider and facility network status before every visit.
• Contact the plan as soon as possible if you do not understand what is covered, if you have any
questions, or if you need information.
• Enroll in Medicare Part A and Part B if you are currently retired, or are in the process of retiring, and
become eligible for Medicare. You must notify the PEBB Program when you enroll in Medicare Part A
and Part B. Call 1-800-200-1004 (TRS: 711) to speak with a customer service representative for the PEBB
Program.
• Follow your providers’ instructions about your health care.
• Give your providers complete information about your health to get the best possible care.
• Keep your mailing address current by reporting changes as follows:
▪ Employees: To your payroll or benefits office.
▪ Retirees, PEBB Continuation Coverage members, and retired employees of a former employer
group: To the PEBB Program. Send your address changes to:
Health Care Authority
PEBB Program
PO Box 42684
Olympia, WA 98504
• Know how to access emergency care.
• Not engage in fraud or abuse in dealing with the plan or your providers.
• Participate with your providers in making decisions about your health care.
• Pay your copays, coinsurance, and deductibles promptly.
• Refund promptly any overpayment made to you or for you.
• Report to the plan any outside sources of health care coverage or payment.
• Return your completed Multiple Coverage Inquiry form you receive from the plan in a timely manner to
prevent delay in claims payment.
• Understand how to contact the plan for more information and help with any covered service or
information described in this COC.
• Understand how UMP coverage coordinates with other insurance coverage you may have, including
Medicare.
• Understand your plan benefits, including what is covered, preauthorization and notice requirements,
and other information described in this COC.
Information available to you
We support the goal of giving you and your family the detailed information you need to make the best
possible health care decisions. See the Directory pages at the beginning of this booklet for links and
contact information):
You may find the following information in this COC:
2024 UMP CDHP (PEBB) Certificate of Coverage 135
• Benefit exclusions, reductions, and maximums or limits (see the “What the plan does not cover” section)
• Clear explanation of complaint and appeal procedures (see the “Complaint and appeal procedures”
section)
• Definition of terms (see the “Definitions” section)
• List of covered expenses (see the “List of benefits” section)
• Policies regarding prescription drug coverage and how the plan adds and removes drugs from the
UMP Preferred Drug List (see “The UMP Preferred Drug List” and the “Guidelines for prescription drugs
UMP covers” sections)
• Preventive health care benefits that are covered (see the “Preventive care” benefit and page 91)
• Process for preauthorization, notice, or review (see the “Limits on plan coverage” section and page 98)
You may find the following on the UMP website, or by contacting UMP Customer Service:
• Accreditation information, including measures used to report the plan’s performance, such as
consumer satisfaction survey results or Healthcare Effectiveness Data and Information Set (HEDIS)
measures
• Clinical coverage criteria applicable to health care services and supplies that require preauthorization
• Description and justification for provider compensation programs, including any incentives or penalties
intended to encourage providers to withhold services
• General reimbursement or payment arrangements between the plan and preferred providers
• Information on the plan’s care management programs
• Notice of privacy practices (includes plan policy for protecting the confidentiality of health information;
see “Confidentiality of your health information” on page 136)
• Online directory of preferred providers, including both primary care providers and specialists
• Procedures to follow for consulting with providers
• The Summary of Benefits and Coverage (SBC)
• When the plan may retroactively deny coverage for preauthorized medical services
The following are available through your Regence account or by contacting UMP Customer Service:
• Medical claims history and deductible status
• Online directory of preferred providers, including both primary care providers and specialists
The following are available on the UMP Prescription drug coverage webpage or by contacting WSRxS
Customer Service:
• The UMP Preferred Drug List
• Clinical coverage criteria applicable to prescription drugs that require preauthorization (through your
online prescription drug account)
• Prescription drug claims history and deductible status (through your online prescription drug account)
You may also contact UMP Customer Service for an annual accounting of all payments made by the plan
that have been counted against medical payment limits, day limits, visit limits, or other limits on your
coverage. The plan will provide a written summary of payments within 30 calendar days of your request.
Some of this information is also available through your Regence account.

136 2024 UMP CDHP (PEBB) Certificate of Coverage
You may contact WSRxS Customer Service with questions about coverage of and limitations on
prescription drugs.
The plan does not prevent or discourage providers from telling you about the care you require, including
various treatment options and whether the provider thinks that care is consistent with the plan’s coverage
criteria. You may, at any time, get health care outside of plan coverage for any reason. However, you must
pay for those services and supplies. In addition, the plan does not prevent or discourage you from talking
about other health plans with your provider.
Confidentiality of your health information
The plan follows the UMP Notice of Privacy Practices, available online on the HCA website at
hca.wa.gov/ump-privacy or by contacting UMP Customer Service. The plan will release member health
information only as described in that notice or as required or permitted by law or court order.
How to designate an authorized representative
TIP: Because of privacy laws, the plan usually cannot share information on appeals or
complaints with family or other persons unless the member is a minor, or the plan has received
written authorization to release personal health information to the other person.
In most cases, the plan must have written authorization to communicate with anyone but the member.
However, a parent or legal guardian may act as a representative for a member under age 13 without
written authorization, except for issues involving contraceptive use. For members ages 13 to 17, a parent
or legal guardian may usually act as a representative, except for certain specially protected types of
information, for which the plan must receive written authorization as described below.
You may choose to authorize a representative to:
• Communicate with the plan on your behalf regarding an appeal in process.
• Share your protected health information.
• Talk to the plan about claims or services.
To authorize release of protected health information, you must complete an Authorization to Disclose
Protected Health Information form. The forms for medical and prescription drug appeals are different. To
get the forms, follow the instructions below:
• Medical benefits: Contact UMP Customer Service or use your Regence account (see Directory for link
and contact information).
• Prescription drug benefits: Contact WSRxS Customer Service or download the UMP (WSRxS)
Prescription drug complaints and appeals form by visiting forms and publications at hca.wa.gov/ump-
forms-pubs.
Send the form to the address on the form. UMP cannot share information until we receive the completed
form. On the form, you must specify:
• What information may be disclosed;
• The purpose of the disclosure (e.g., receiving an outcome of an appeal); and
• Who is designated to receive or release the information.
2024 UMP CDHP (PEBB) Certificate of Coverage 137
Release of information
The plan or HCA may require you to give information when needed to determine eligibility, administer
benefits, or process claims. This could include medical and other records. The plan could deny coverage if
you do not provide the information when requested.
Relationship to Blue Cross and Blue Shield Association
HCA, on behalf of itself and its members, hereby expressly acknowledges that this contract constitutes an
agreement solely between HCA and Regence BlueShield, an independent corporation operating under a
license from the Blue Cross and Blue Shield Association, an association of independent Blue Cross and
Blue Shield plans (the “Association”), permitting the contractor Regence BlueShield to use the Washington
license for those counties designated in its service area.
Right to receive and release needed information
Regence BlueShield may need certain facts about your health care coverage or services provided to
process your claims correctly. Regence may get these facts from or give them to other organizations or
persons without your consent. You must give Regence any facts necessary for processing of claims to get
benefits under this plan. See page 136 for more information about the confidentiality of your health
information.
Right of recovery
The plan has the right to a refund of incorrect payments. The plan may recover excess payment from any:
• Person that received an excess payment.
• Person on whose behalf an excess payment was made.
• Other issuers of payment.
• Other plans involved.
Limitations on liability
In all cases, you have the exclusive right to choose a health care provider. Since neither UMP nor Regence
BlueShield provides any health care services, neither may be held liable for any claim or damages
connected with injuries you may suffer while receiving health services or supplies provided by
professionals who are neither employees nor agents of either UMP or Regence BlueShield. Neither
Regence BlueShield nor UMP is responsible for the quality of health care you receive, except as provided
by law.
In addition, UMP will not be liable to any person or entity for the inability or failure to procure or provide
the benefits of the plan by reason of epidemic, disaster, or other cause or condition beyond UMP’s
control.
Governing law
The plan is governed by and construed in accordance with the laws of the United States of America and
by applicable laws of Washington State without regard to its conflict of law rules.
Anti-assignment
Members may not assign this COC, or any rights, interests or obligations contained in this COC, in whole
or in part, to a third party (including, but not limited to, providers of medical services), without the plan’s
138 2024 UMP CDHP (PEBB) Certificate of Coverage
written consent. Any attempt to assign any rights, interests or obligations contained in this COC, in whole
or in part, to a third party is void and/or invalid, and the plan will not recognize it.
No waiver
The failure or refusal of either party to demand strict performance of the plan or to enforce any provision
will not act as or be construed as a waiver of that party’s right to later demand its performance or to
enforce that provision. No provision of the plan will be considered waived unless such waiver is in writing
and signed by one of HCA’s authorized officers.
2024 UMP CDHP (PEBB) Certificate of Coverage 139
Acronyms
ABA – Applied Behavior Analysis [Therapy]
ACP – Accountable Care Program
ASC – Ambulatory surgery center
CDC – Centers for Disease Control and
Prevention
CDHP – Consumer-directed health plan
CHIP – Children’s Health Insurance Program
CMS – Centers for Medicare and Medicaid
Services
COB – Coordination of benefits
COBRA – Consolidated Omnibus Budget
Reconciliation Act
COC – Certificate of coverage
COE – Centers of Excellence Program
DME – Durable medical equipment
DPP – Diabetes Prevention Program
EOB – Explanation of benefits
EOMB – Explanation of Medicare benefits
ER – Emergency room
ERB – Employee and Retiree Benefits [Division]
FDA – Food and Drug Administration
FMLA – Family Medical Leave Act
FSA – Flexible spending arrangement
HCA – Health Care Authority
HDHP – High-deductible health plan
HIPAA – Health Insurance Portability and
Accountability Act
HRA – Health reimbursement arrangement
HRSA – Health Resources and Services
Administration
HSA – Health savings account
HTCC – Health Technology Clinical Committee
IRC – Internal Revenue Code
IRO – Independent review organization
IRS – Internal Revenue Service
MSN – Medicare Summary Notice
NMSN – National Medical Support Notice
P – Preventive
P&T – Pharmacy and Therapeutics Committee
PCP – Primary care provider
PEBB – Public Employees Benefits Board
PFML – Paid Family and Medical Leave
PPACA – Patient Protection and Affordable Care
Act
PPO – Preferred Provider Organization
PPS – Postal Prescription Services
RCW – Revised Code of Washington
REMS – Risk Evaluation and Mitigation Strategies
SBC – Summary of Benefits and Coverage
SEBB – School Employees Benefits Board
TMJ – Temporomandibular joint
TRS – Telecommunications Relay Service
UMP – Uniform Medical Plan
V – Value tier
WAC – Washington Administrative Code
WSRxS – Washington State Rx (prescription
drug) Services
140 2024 UMP CDHP (PEBB) Certificate of Coverage
Eligibility and enrollment
In these sections, “health plan” is used to refer to a plan offering medical or dental, or both, developed by
the Public Employees Benefits Board (PEBB) and provided by a contracted vendor or self-insured plans
administered by the Health Care Authority (HCA).
Eligibility for subscribers and dependents
Employee eligibility
The employee’s state agency will inform the employee in writing whether or not they are eligible for PEBB
benefits upon employment and whenever their eligibility status changes. The written notice will include
information about the employee’s right to appeal eligibility and enrollment decisions.
An employee of an employer group (such as a county, city, port, water district, etc.) that contracts with
HCA for PEBB benefits should contact their payroll or benefits office for eligibility criteria.
Employees have the right to appeal eligibility and enrollment decisions. Information about appeals can be
found under “Appeal rights.”
Continuation coverage eligibility
The PEBB Program determines whether subscribers are eligible for continuation coverage (COBRA or
Unpaid Leave) upon receipt of their election to enroll in PEBB Continuation Coverage (COBRA or Unpaid
Leave). If the subscriber requests to enroll in and is not eligible for continuation coverage, the PEBB
Program will notify them of their right to appeal. Information about appeals can be found under “Appeal
rights.”
Retired employee of a former employer group eligibility
The PEBB Program determines whether a retired employee or a retired school employee of a former
employer group is eligible to self-pay coverage upon receipt of their election to enroll. If the retired
employee or the retired school employee requests to enroll and is not eligible, the PEBB Program will
notify them of their right to appeal. Information about appeals can be found under “Appeal rights.”
Dependent eligibility
The following are eligible dependents:
• Legal spouse
• State-registered domestic partner and substantially equivalent legal unions from jurisdictions as
defined in Washington State statute. Individuals in a state-registered domestic partnership are treated
the same as a legal spouse except when in conflict with federal law.
• Children, through the last day of the month in which their 26th birthday occurred regardless of marital
status, student status, or eligibility for coverage under another plan. It also includes children age 26 or
older with a disability as described below in “Children of any age with a developmental or physical
disability.” Children are defined as the subscriber’s:
▪ Children based on establishment of a parent-child relationship, as described in Washington
State statutes, except when parental rights have been terminated.
▪ Children of the subscriber’s spouse, based on the spouse’s establishment of a parent-child
relationship, except when parental rights have been terminated. The stepchild’s relationship to the
subscriber (and eligibility as a dependent) ends on the same date the marriage with the spouse ends
through divorce, annulment, dissolution, termination, or death.
2024 UMP CDHP (PEBB) Certificate of Coverage 141
▪ Children for whom the subscriber has assumed a legal obligation for total or partial support in
anticipation of adoption of the child.
▪ Children of the subscriber’s state-registered domestic partner, based on the state-registered
domestic partner’s establishment of a parent-child relationship, except when parental rights have
been terminated. The child’s relationship to the subscriber (and eligibility as a dependent) ends on
the same date the subscriber’s legal relationship with the state-registered domestic partner ends
through divorce, annulment, dissolution, termination, or death.
▪ Children specified in a court order or divorce decree for whom the subscriber has a legal
obligation to provide support or health care coverage.
▪ Extended dependents in the legal custody or legal guardianship of the subscriber, the
subscriber’s spouse, or the subscriber’s state-registered domestic partner. The legal
responsibility is demonstrated by a valid court order and the child’s official residence with the
custodian or guardian. Extended dependent child does not include foster children unless the
subscriber, the subscriber’s spouse, or the subscriber’s state-registered domestic partner has
assumed a legal obligation for total or partial support in anticipation of adoption.
▪ Children of any age with a developmental or physical disability that renders them incapable of
self-sustaining employment and chiefly dependent upon the subscriber for support and
maintenance, provided such condition occurs before the age of 26. The following requirements
apply to a dependent child with a disability:
◦ The subscriber must provide proof of the disability and dependency within 60 days of the child’s
attainment of age 26.
◦ The subscriber must notify the PEBB Program in writing when the child is no longer eligible under
this subsection.
◦ A child with a developmental or physical disability who becomes self-supporting is not eligible as
of the last day of the month in which they become capable of self-support.
◦ A child with a developmental or physical disability age 26 and older who becomes capable of self-
support does not regain eligibility if they later become incapable of self-support.
◦ The PEBB Program, with input from the medical plan, will periodically verify the eligibility of a
dependent child with a disability beginning at age 26, but no more frequently than annually after
the two-year period following the child’s 26th birthday. Verification will require renewed proof of
disability and dependence from the subscriber.
Enrollment for subscribers and dependents
For all subscribers and dependents
• To enroll at any time other than during the initial enrollment period, see “Making changes.”
• Any dependents enrolled in medical coverage will be enrolled in the same medical plan as the
subscriber. Exceptions apply for non-Medicare enrollees when a subscriber selects a Medicare
Supplement, Medicare Advantage, or Medicare Advantage Prescription Drug plan.
Employee enrollment
An employee must use Benefits 24/7, the online enrollment system (once available), or submit a PEBB
Employee Enrollment/Change or PEBB Employee Enrollment/Change (for Medical Only Groups) form and
any supporting documents to their employing agency when they become newly eligible or regain
eligibility for PEBB benefits. The online enrollment must be completed or the form must be received no
later than 31 days after the date the employee becomes eligible or regains eligibility.

142 2024 UMP CDHP (PEBB) Certificate of Coverage
If the employee does not enroll online or return the form by the deadline, the employee will be enrolled in
Uniform Medical Plan Classic and a tobacco use premium surcharge will be incurred. Consequently,
dependents cannot be enrolled until the PEBB Program’s next annual open enrollment or when a
qualifying event occurs that creates a special open enrollment for enrolling a dependent.
Waiving medical enrollment
An eligible employee may waive enrollment in PEBB medical if they are enrolled in other employer-based
group medical, a TRICARE plan, or Medicare. They may not waive enrollment in PEBB medical if they are
enrolled in PEBB retiree insurance coverage. When a retiree becomes eligible for the employer
contribution toward PEBB benefits, PEBB retiree insurance coverage will be automatically deferred.
If an employee waives enrollment in PEBB medical, the employee cannot enroll eligible dependents. For
information on when an eligible employee may waive medical plan enrollment after their initial
enrollment period, or to enroll after having waived, see “Making changes.”
Continuation coverage enrollment
A subscriber enrolling in PEBB Continuation Coverage (COBRA or Unpaid Leave) may enroll by using
Benefits 24/7, the online enrollment system (once available), or by submitting the applicable PEBB
Continuation Coverage Election/Change form and any supporting documents to the PEBB Program. The
online enrollment must be completed or the PEBB Program must receive the election form no later than
60 days from the date the enrollee’s PEBB health plan coverage ended or from the postmark date on the
PEBB Continuation Coverage Election Notice sent by the PEBB Program, whichever is later.
Premiums and applicable premium surcharges associated with continuing PEBB medical must be made
directly to HCA. The first premium payment and applicable premium surcharges are due to HCA no later
than 45 days after the election period ends as described above. For more information, see “Options for
continuing PEBB medical coverage” and the PEBB Continuation Coverage Election Notice.
Retired employee of a former employer group enrollment
A retired employee or a retired school employee of a former employer group may enroll and self-pay
premiums using Benefits 24/7, the online enrollment system (once available), or by submitting the PEBB
Continuation Coverage (Employer Group Ended Participation) Election/Change form and any supporting
documents to the PEBB Program. The online enrollment must be completed or the PEBB Program must
receive the required form no later than 60 days after the employer group ended their participation.
Premiums and applicable premium surcharges associated with continuing PEBB medical must be made
directly to HCA. The first premium payment and applicable premium surcharges are due to HCA no later
than 45 days after the election period ends as described above.
Note: Enrollment in the PEBB Program’s Medicare Advantage Prescription Drug (MAPD) plan may not be
retroactive. If a subscriber elects a MAPD plan and the online enrollment or the required forms are
received by the PEBB Program after the date PEBB health plan coverage is to begin, the subscriber and
their enrolled dependents will be enrolled in the Uniform Medical Plan Classic during the gap month(s)
prior to when the MAPD plan begins.
Dependent enrollment
To enroll an eligible dependent, the subscriber must include the dependent’s information online using
Benefits 24/7 (once available) or on the applicable enrollment form and provide the required document(s)
as proof of the dependent’s eligibility. The dependent will not be enrolled in PEBB health plan coverage if
the PEBB Program or the employing agency is unable to verify their eligibility within the PEBB Program
enrollment timelines.
2024 UMP CDHP (PEBB) Certificate of Coverage 143
National Medical Support Notice (NMSN)
When a National Medical Support Notice (NMSN) requires a subscriber to provide health plan coverage
for a dependent child, the following provisions apply:
The subscriber may enroll their dependent child and request changes to their health plan coverage as
described under “Changes to health plan coverage or enrollment are allowed as directed by the NMSN,”
below.
• An employee must use Benefits 24/7 (once available) or submit the required form(s) to their
employing agency.
• Any other subscriber must use Benefits 24/7 (once available) or submit the required form(s) to the
PEBB Program.
If the subscriber fails to request enrollment or health plan coverage changes as directed by the NMSN, the
employing agency or the PEBB Program may make enrollment or health plan coverage changes according
to “Changes to health plan coverage or enrollment are allowed as directed by the NMSN,” below, upon
request of:
• The child’s other parent.
• A child support enforcement program.
Changes to health plan coverage or enrollment are allowed as directed by the NMSN:
A. The dependent will be enrolled under the subscriber’s health plan coverage as directed by the
NMSN.
B. An employee who has waived PEBB medical will be enrolled in medical as directed by the NMSN,
in order to enroll the dependent.
C. The subscriber’s selected health plans will be changed if directed by the NMSN.
D. If the dependent is already enrolled under another PEBB subscriber, the dependent will be
removed from the other health plan coverage and enrolled as directed by the NMSN.
E. If the dependent is enrolled in both PEBB medical and School Employee Benefits Board (SEBB)
medical as a dependent and there is an NMSN in place, enrollment will be in accordance with the
NMSN.
F. If the subscriber is eligible for and elects Consolidated Omnibus Budget Reconciliation Act
(COBRA) coverage or other continuation coverage, the NMSN will be enforced and the dependent
must be covered in accordance with the NMSN.
Changes to health plan coverage or enrollment as described above in A through C will begin the first day
of the month following receipt of the NMSN. If the NMSN is received on the first day of the month, the
change to health plan coverage or enrollment begins on that day.
A dependent will be removed from the subscriber’s health plan coverage as described above in D the last
day of the month the NMSN is received. If that day is the first of the month, the change in enrollment will
be made the last day of the previous month.
When a NMSN requires a subscriber’s spouse, former spouse, or other individual to provide health plan
coverage for a dependent who is already enrolled in the subscriber’s PEBB coverage, and that health plan
coverage is in fact provided, the dependent may be removed from the subscriber’s PEBB health plan
coverage prospectively.
Dual enrollment
A subscriber and their dependents may each be enrolled in only one PEBB medical plan.
144 2024 UMP CDHP (PEBB) Certificate of Coverage
An employee or their dependent who is eligible to enroll in both the PEBB Program and the School
Employees Benefits Board (SEBB) Program is limited to a single enrollment in either the PEBB or SEBB
Program.
For example:
• A child who is an eligible dependent under two parents enrolled in PEBB Program benefits may be
enrolled as a dependent under both parents but is limited to a single enrollment in PEBB medical.
• A child who is an eligible dependent of an employee in the PEBB Program and a school employee in
the SEBB Program may only be enrolled as a dependent under one parent in either the PEBB or SEBB
Program.
Medicare eligibility and enrollment
Employee and dependent
If an employee or their dependent becomes eligible for Medicare, they should contact the Social Security
Administration to ask about the advantages of immediate or deferred Medicare enrollment.
An employee or their dependent are deemed eligible for Medicare when they have the option to receive
Medicare Part A benefits. If an employee or their dependent chooses to enroll in Medicare Part A,
Medicare regulations and guidelines will determine whether Medicare is the primary or secondary payer.
An employee or their dependent who is enrolled in Medicare may remain enrolled in PEBB medical
coverage. However, an employee may choose to waive their PEBB medical coverage or remove their
dependent from their PEBB medical coverage and choose Medicare as their primary insurer. If an
employee does so, neither the employee nor their dependent can enroll in PEBB medical except during
the annual open enrollment or a special open enrollment.
In most situations, an employee and their dependent can defer Medicare Part B enrollment without a
penalty while enrolled in PEBB medical coverage. When the employee terminates employment, the
employee and the dependent can enroll in Medicare Part B during a Special Enrollment Period. If
Medicare eligibility is due to a disability, the employee or their dependent must contact the Social
Security Administration about deferring enrollment in Medicare Part B.
Upon retirement, Medicare will become the primary insurance payer, and the PEBB medical plan will
become secondary. See “PEBB retiree insurance coverage.”
Continuation coverage subscriber, a retired employee of a
former employer group, or their dependent
If a continuation coverage subscriber, a retired employee of a former employer group, or their
dependent becomes eligible for Medicare, federal regulations allow enrollment in Medicare three months
before they turn age 65. If they do not enroll within three months before the month they turn age 65,
enrollment in Medicare may be delayed. If enrollment in Medicare does not occur when the subscriber or
their dependent is first eligible, a late enrollment penalty may apply.
When medical coverage begins
Employees and dependents
For a newly eligible employee and their eligible dependents, medical coverage begins the first day of
the month following the date the employee becomes eligible. If the employee becomes eligible on the
first working day of the month, then coverage begins on that date.
2024 UMP CDHP (PEBB) Certificate of Coverage 145
If the eligible employee is a faculty member hired on a quarter-to-quarter or semester-to-semester basis,
medical coverage begins the first day of the month following the beginning of the second consecutive
quarter or semester. If the first day of the second consecutive quarter or semester is the first working day
of the month, medical coverage begins on that day.
For an employee regaining eligibility, including following a period of leave or after being between
periods of leave as described in PEBB Program rules, and their eligible dependents, medical coverage
begins the first day of the month the employee is in pay status eight or more hours. If the employee is a
faculty member regaining eligibility no later than the 12th
month after the month in which they lost
eligibility for the employer contribution toward PEBB benefits, medical coverage begins the first day of the
month in which the quarter or semester begins.
Note: When an employee who is called to active duty in the uniformed services under the Uniformed
Services Employment and Reemployment Rights Act (USERRA) loses eligibility for the employer
contribution toward PEBB benefits, they regain eligibility for the employer contribution toward PEBB
benefits the day they return from active duty. Medical coverage begins the first day of the month in which
the employee returns from active duty.
Continuation coverage subscribers and dependents
For a continuation coverage subscriber and their eligible dependents enrolling when newly eligible due
to a qualifying event, medical coverage begins the first day of the month following the day they lost
eligibility for PEBB medical plan coverage.
Retired employees of a former employer group and dependents
For a retired employee of a former employer group and their eligible dependents enrolling when
newly eligible, medical coverage begins the first day of the month following the day they lost eligibility for
PEBB retiree insurance coverage.
All subscribers and dependents
For a subscriber or their eligible dependents enrolling during the PEBB Program’s annual open
enrollment, medical coverage begins January 1 of the following year.
For a subscriber or their eligible dependents enrolling during a special open enrollment, medical
coverage begins the first day of the month following the later of the event date or the date the online
enrollment election using Benefits 24/7 (once available) or the required form is received. If that day is the
first of the month, medical coverage begins on that day, except for a Medicare Advantage or Medicare
Advantage Prescription Drug plan, which will begin the first day of the month following the date the
enrollment election is received online or the required form is received by the PEBB Program.
If the special open enrollment is due to the birth or adoption of a child, or when the subscriber has
assumed a legal obligation for total or partial support in anticipation of adoption of a child, medical
coverage will begin as follows:
• For an employee, medical coverage will begin the first day of the month in which the event occurs.
• For a newly born child, medical coverage will begin the date of birth.
• For a newly adopted child, medical coverage will begin on the date of placement or the date a legal
obligation is assumed in anticipation of adoption, whichever is earlier.
• For a spouse or state-registered domestic partner of a subscriber, medical coverage will begin the
first day of the month in which the event occurs.
146 2024 UMP CDHP (PEBB) Certificate of Coverage
If the special open enrollment is due to the enrollment of an extended dependent or a dependent child
with a disability, medical coverage will begin the first day of the month following the event date or
eligibility certification, whichever is later.
Making changes
Removing a dependent who is no longer eligible
A subscriber must provide notice to remove a dependent who is no longer eligible due to divorce,
annulment, dissolution, or a qualifying event of a dependent ceasing to be eligible as a dependent child
as described under “Dependent eligibility.” The notice must be received within 60 days of the last day of
the month the dependent no longer meets the eligibility criteria.
• An employee must provide notice online using Benefits 24/7 (once available) or by submitting a
written request to their employing agency.
• Any other subscriber must provide notice online using Benefits 24/7 (once available) or by submitting
a written request to the PEBB Program.
Consequences for not submitting notice within the required 60 days may include, but are not limited to:
• The dependent may lose eligibility to continue PEBB medical coverage under one of the continuation
coverage options described in “Options for continuing PEBB medical coverage.”
• The subscriber may be billed for claims paid by the medical plan for services that were rendered after
the dependent lost eligibility.
• The subscriber may not be able to recover subscriber-paid insurance premiums for the dependent that
lost eligibility.
• The subscriber may be responsible for premiums paid by the state for the dependent’s medical plan
coverage after the dependent lost eligibility.
Voluntary termination for continuation coverage subscribers
or retired employees of a former employer group
A continuation coverage subscriber or a retired employee of a former employer group may voluntarily
terminate enrollment in a medical plan at any time by submitting a request online using Benefits 24/7
(once available) or in writing to the PEBB Program. Enrollment in the medical plan will be terminated the
last day of the month in which the request was received online or by the PEBB Program, or on the last day
of the month specified in the termination request, whichever is later. If the request is received on the first
day of the month, medical plan enrollment will be terminated on the last day of the previous month.
Exception: When a subscriber or their dependent is enrolled in a Medicare Advantage or Medicare
Advantage Prescription Drug plan, then medical plan enrollment will terminate on the last day of the
month when the PEBB Medicare Advantage Plan Disenrollment form (form D) is received.
Making changes during annual open enrollment and special
open enrollment
A subscriber may make certain changes to their enrollment during the annual open enrollment and if a
specific life event creates a special open enrollment period.
Annual open enrollment changes
An employee may make the following changes to their enrollment during the PEBB Program’s annual
open enrollment period:
• Change their medical plan

2024 UMP CDHP (PEBB) Certificate of Coverage 147
• Waive their medical plan enrollment
• Enroll after waiving medical plan enrollment
• Enroll or remove eligible dependents
An employee must submit the election change online using PEBB My Account or Benefits 24/7 (once
available) or submit the required PEBB Employee Enrollment/Change form and any supporting documents
to their employing agency. The change must be completed online, or the forms received, no later than the
last day of the annual open enrollment period and will be effective January 1 of the following year.
Any other subscriber may make the following changes to their enrollment during the PEBB Program’s
annual open enrollment period:
• Enroll in or terminate enrollment in a medical plan
• Change their medical plan
• Enroll or remove eligible dependents
A continuation coverage subscriber must submit the election change online using PEBB My Account or
Benefits 24/7 (once available) or submit the required PEBB Continuation Coverage (COBRA)
Election/Change, or PEBB Continuation Coverage (Unpaid Leave) Election/Change form (as appropriate)
and any supporting documents to the PEBB Program. The change must be completed online, or the forms
received, no later than the last day of the annual open enrollment period and will be effective January 1 of
the following year.
A retired employee of a former employer group must submit the election change online using PEBB
My Account or Benefits 24/7 (once available) or submit the required PEBB Continuation Coverage
(Employer Group Ended Participation) Election/Change form and any supporting documents to the PEBB
Program. The change must be completed online, or the forms received, no later than the last day of the
annual open enrollment period and will be effective January 1 of the following year.
Special open enrollment changes
A subscriber may change their enrollment outside of the annual open enrollment period if a qualifying
event creates a special open enrollment period. However, the change in enrollment must be allowable
under Internal Revenue Code (IRC) and Treasury Regulations and correspond to and be consistent with
the event that creates the special open enrollment for the subscriber, their dependent, or both.
A special open enrollment event must be other than an employee gaining initial eligibility or regaining
eligibility for PEBB benefits. The subscriber must provide evidence of the event that created the special
open enrollment.
A special open enrollment may allow a subscriber to make the following changes:
• Enroll in or change their medical plan
• Waive their medical plan enrollment
• Enroll after waiving medical plan enrollment
• Enroll or remove eligible dependents
To request a special open enrollment:
• An employee must make the change online using Benefits 24/7 (once available) or submit the required
PEBB Employee Enrollment/Change form and any supporting documents to their employing agency.
• A continuation coverage subscriber must make the change online using Benefits 24/7 (once
available) or submit the required PEBB Continuation Coverage (COBRA) Election/Change, or PEBB
148 2024 UMP CDHP (PEBB) Certificate of Coverage
Continuation Coverage (Unpaid Leave) Election/Change form (as appropriate) and any supporting
documents to the PEBB Program.
• A retired employee of a former employer group must make the change online using Benefits
24/7 (once available) or submit the required PEBB Continuation Coverage (Employer Group
Ended Participation) Election/Change form and any supporting documents to the PEBB Program.
The change must be completed online, or the forms must be received, no later than 60 days after the
event that creates the special open enrollment. In addition, the PEBB Program or the employing agency
will require the subscriber to provide proof of a dependent’s eligibility, evidence of the event that created
the special open enrollment, or both.
Exceptions:
• If a subscriber wants to enroll a newborn or child whom the subscriber has adopted or has assumed a
legal obligation for total or partial support in anticipation of adoption in PEBB health plan coverage,
the subscriber should complete the request online or notify their employing agency or the PEBB
Program by submitting the required forms as soon as possible to ensure timely payment of claims. If
adding the child increases the premium, the request must be received online, or the required forms
must be received, no later than 60 days after the date of the birth, adoption, or the date the legal
obligation is assumed for total or partial support in anticipation of adoption.
A continuation coverage subscriber or a retired employee of a former employer group:
• Has six months from the date of their or their dependent’s enrollment in Medicare Part B to change
their enrollment to a PEBB Medicare Supplement Plan. The change must be made online using Benefits
24/7 (once available) or the PEBB Program must receive the required form(s) no later than six months
after the enrollment in Medicare Part B for either the subscriber or their dependent.
• When they or their dependent is enrolled in a Medicare Advantage (MA) or Medicare Advantage
Prescription Drug (MAPD) plan, they may disenroll during a special enrollment period as allowed under
federal regulations. The new medical plan coverage will begin the first day of the month following the
date the PEBB Medicare Advantage Plan Disenrollment Form (form D) is received.
• Has seven months to enroll in an MA or MAPD plan that begins three months before they or their
dependent first enrolled in both Medicare Part A and Part B and ends three months after the month of
Medicare eligibility. They may also enroll themselves or their dependent in an MA or MAPD plan
before their last day of the Medicare Part B initial enrollment period. The change must be made online
in Benefits 24/7 (once available), or the forms must be received by the PEBB Program, no later than the
last day of the month prior to the month they or their dependent enrolls in the MA or MAPD plan.
Special open enrollment events that allow for a change in health plans
A subscriber may not change their health plan during a special open enrollment if their state-registered
domestic partner or state-registered domestic partner’s child is not a tax dependent.
Any of the following events may create a special open enrollment:
• Subscriber gains a new dependent due to:
▪ Marriage or registering a state-registered domestic partnership.
▪ Birth, adoption, or assuming a legal obligation for total or partial support in anticipation of adoption.
▪ A child becoming eligible as an extended dependent through legal custody or legal guardianship.
• Subscriber or their dependent loses other coverage under a group health plan or through health
insurance coverage, as defined by the Health Insurance Portability and Accountability Act (HIPAA).
2024 UMP CDHP (PEBB) Certificate of Coverage 149
• Subscriber has a change in employment status that affects their eligibility for the employer contribution
toward their employer-based group health plan.
• Subscriber’s dependent has a change in their own employment status that affects their eligibility or
their dependent’s eligibility for the employer contribution under their employer-based group health
plan. “Employer contribution” means contributions made by the dependent’s current or former
employer toward health coverage as described in the Treasury Regulation.
• Subscriber or their dependent has a change in residence that affects health plan availability. If the
subscriber has a change in residence and their current medical plan is no longer available, the
subscriber must select a new medical plan as described in PEBB Program rules. If the subscriber does
not elect a new medical plan as required, they will be enrolled in a PEBB medical plan designated by
the director of HCA or their designee.
• A court order requires the subscriber or any other individual to provide insurance coverage for an
eligible dependent of the subscriber (a former spouse or former state-registered domestic partner is
not an eligible dependent).
• Subscriber or their dependent enrolls in coverage under Medicaid or a state Children’s Health
Insurance Program (CHIP), or the subscriber or their dependent loses eligibility for coverage under
Medicaid or CHIP.
• Subscriber or their dependent becomes eligible for state premium assistance subsidy for PEBB health
plan coverage from Medicaid or CHIP.
• Subscriber or their dependent enrolls in coverage under Medicare, or the subscriber or their dependent
loses eligibility for coverage under Medicare or enrolls in or terminates enrollment in a Medicare
Advantage Prescription Drug or a Part D plan. If the subscriber’s current medical plan becomes
unavailable due to the subscriber or their dependents enrollment in Medicare, the subscriber must
select a new medical plan.
• Subscriber or their dependent’s current medical plan becomes unavailable because the subscriber or
enrolled dependent is no longer eligible for a health savings account (HSA).
• Subscriber or their dependent experiences a disruption of care for active and ongoing treatment that
could function as a reduction in benefits for the subscriber or their dependent. The subscriber may not
change their health plan election because the subscriber or dependent’s physician stops participation
with the subscriber’s health plan unless the PEBB Program determines that a continuity of care issue
exists. The PEBB Program will consider but not limit its consideration to the following:
▪ Active cancer treatment, such as chemotherapy or radiation therapy
▪ Treatment following a recent organ transplant
▪ A scheduled surgery
▪ Recent major surgery still within the postoperative period
▪ Treatment for a high-risk pregnancy
▪ The PEBB Program determines that there has been a substantial decrease in the providers available
under a PEBB medical plan.
Note: The plan cannot guarantee that any physician, hospital, or other provider will be available or remain
under contract with the plan. An enrollee may not change medical plans simply because their provider or
health care facility discontinues participation with this medical plan until the PEBB Program’s next annual
open enrollment or when another qualifying event creates a special open enrollment for changing health
plans, unless the PEBB Program determines that a continuity of care issue exists or there has been a
substantial decrease in the providers available under the plan.
150 2024 UMP CDHP (PEBB) Certificate of Coverage
Special open enrollment events that allow adding or removing a dependent
Any of the following events may create a special open enrollment:
• Subscriber gains a new dependent due to:
▪ Marriage or registering a state-registered domestic partnership.
▪ Birth, adoption, or when the subscriber has assumed a legal obligation for total or partial support in
anticipation of adoption.
▪ A child becoming eligible as an extended dependent through legal custody or legal guardianship.
• Subscriber or their dependent loses other coverage under a group health plan or through health
insurance coverage, as defined by the Health Insurance Portability and Accountability Act (HIPAA).
• Subscriber has a change in employment status that affects their eligibility for the employer contribution
toward their employer-based group health plan.
• Subscriber’s dependent has a change in their own employment status that affects their eligibility or
their dependent’s eligibility for the employer contribution under their employer-based group health
plan. “Employer contribution” means contributions made by the dependent’s current or former
employer toward health coverage as described in the Treasury Regulation.
• Subscriber or their dependent has a change in enrollment under an employer-based group health plan
during its annual open enrollment that does not align with the PEBB Program’s annual open
enrollment.
• Subscriber’s dependent has a change in residence from outside of the United States to within the
United States, or from within the United States to outside of the United States and that change in
residence resulted in the dependent losing their health insurance.
• A court order requires the subscriber or any other individual to provide insurance coverage for an
eligible dependent of the subscriber (a former spouse or former state-registered domestic partner is
not an eligible dependent).
• Subscriber or their dependent enrolls in coverage under Medicaid or a state Children’s Health
Insurance Program (CHIP), or the subscriber or their dependent loses eligibility for coverage under
Medicaid or CHIP.
• Subscriber or their dependent becomes eligible for a state premium assistance subsidy for PEBB health
plan coverage from Medicaid or CHIP.
• Subscriber’s dependent enrolls in Medicare or loses eligibility for Medicare.
Special open enrollment events that allow waiving medical enrollment and
enrolling after waiving
An employee may waive PEBB medical during a special open enrollment if they are enrolled in other
employer-based group medical, a TRICARE plan, or Medicare. An employee may not waive enrollment in
PEBB medical if they are enrolled in PEBB retiree insurance coverage.
Any of the following events may create a special open enrollment:
• Employee gains a new dependent due to:
▪ Marriage or registering a state-registered domestic partnership.
▪ Birth, adoption, or when the employee has assumed a legal obligation for total or partial support in
anticipation of adoption.
▪ A child becoming eligible as an extended dependent through legal custody or legal guardianship.
2024 UMP CDHP (PEBB) Certificate of Coverage 151
• Employee or their dependent loses other coverage under a group health plan or through health
insurance coverage, as defined by the HIPAA.
• Employee has a change in employment status that affects their eligibility for the employer contribution
toward their employer-based group medical.
• Employee’s dependent has a change in their own employment status that affects their eligibility or their
dependent’s eligibility for the employer contribution under their employer-based group medical.
“Employer contribution” means contributions made by the dependent’s current or former employer
toward health coverage as described in the Treasury Regulation.
• Employee or their dependent has a change in enrollment under an employer-based group medical plan
during its annual open enrollment that does not align with the PEBB Program’s annual open
enrollment.
• Employee’s dependent has a change in residence from outside of the United States to within the
United States, or from within the United States to outside of the United States and the change in
residence resulted in the dependent losing their health insurance.
• A court order requires the employee or any other individual to provide a health plan for an eligible
dependent of the employee (a former spouse or former state-registered domestic partner is not an
eligible dependent).
• Employee or their dependent enrolls in coverage under Medicaid or a state Children’s Health Insurance
Program (CHIP), or the employee or their dependent loses eligibility for coverage under Medicaid or
CHIP. Note: An employee may only return from having waived PEBB medical for the events described
in this paragraph. An employee may not waive their PEBB medical for the events described in this
paragraph.
• Employee or their dependent becomes eligible for a state premium assistance subsidy for PEBB health
plan coverage from Medicaid or CHIP.
• Employee or their dependent becomes eligible and enrolls in a TRICARE plan, or loses eligibility for a
TRICARE plan.
• Employee becomes eligible and enrolls in Medicare or loses eligibility for Medicare.
When medical coverage ends
Termination dates
Medical coverage ends on the following dates:
• On the last day of the month when any enrollee ceases to be eligible.
• On the date a medical plan terminates due to a change in contracted service area or when the group
policy ends. If that should occur, the subscriber will have the opportunity to enroll in another PEBB
medical plan.
• For an employee and their dependents, on the last day of the month the employment relationship is
terminated. The employment relationship is considered terminated:
▪ On the date specified in an employee’s letter of resignation.
▪ On the date specified in any contract or hire letter.
▪ On the effective date of an employer-initiated termination notice.
Note: If the employing agency deducted the employee’s premium for PEBB insurance coverage after the
employee was no longer eligible for the employer contribution, medical coverage ends the last day of the
month for which employee premiums were deducted.
152 2024 UMP CDHP (PEBB) Certificate of Coverage
• For a continuation coverage subscriber or a retired employee of a former employer group who
submits a request to terminate medical coverage, enrollment in medical coverage will be terminated
the last day of the month in which the request was received online using Benefits 24/7 (once available)
or by the PEBB Program, or on the last day of the month specified in the termination request,
whichever is later. If the request is received on the first day of the month, medical coverage will be
terminated on the last day of the previous month.
Exception: When a subscriber or their dependent is enrolled in a Medicare Advantage or Medicare
Advantage Prescription Drug plan, the medical plan enrollment will terminate on the last day of the
month when the PEBB Medicare Advantage Plan Disenrollment form (form D) is received.
A subscriber will be responsible for payment of any services received after the date medical coverage
ends as described above.
Final premium payments
Premium payments and applicable premium surcharges are not prorated during any month, for any
reason, even if an enrollee dies or asks to terminate their medical plan before the end of the month.
If the monthly premium or applicable premium surcharges remain unpaid for 30 days, the account will be
considered delinquent. A subscriber is allowed a grace period of 30 days from the date the monthly
premiums or applicable premium surcharges become delinquent to pay the unpaid premium balance and
applicable premium surcharges. If the subscriber’s premium balance or applicable premium surcharges
remain unpaid for 60 days from the original due date, the subscriber’s medical coverage (including
enrolled dependents) will be terminated retroactive to the last day of the month for which the monthly
premiums and any applicable premium surcharges were paid.
For a subscriber enrolled in a Medicare Advantage or a Medicare Advantage-Prescription Drug plan, a
notice will be sent notifying them that they are delinquent on their monthly premium and that the
enrollment will be terminated prospectively to the end of the month after the notice is sent.
If an enrollee is hospitalized
An enrollee who is receiving covered services in a hospital on the date medical coverage ends will
continue to be eligible for covered services while an inpatient for the condition which the enrollee was
hospitalized, until one of the following events occur:
• According to this plan’s clinical criteria, it is no longer medically necessary for the enrollee to be an
inpatient at the facility.
• The remaining benefits available for the hospitalization are exhausted, regardless of whether a new
calendar year begins.
• The enrollee becomes covered under another agreement with a group health plan that provides
benefits for the hospitalization.
• The enrollee becomes enrolled under an agreement with another carrier that provides benefits for the
hospitalization.
This provision will not apply if the enrollee is covered under another agreement that provides benefits for
the hospitalization at the time medical coverage ends, except as set forth in this section, or if the enrollee
is eligible for PEBB Continuation Coverage as described in “Options for continuing PEBB medical
coverage.”
Options for continuing PEBB medical coverage
When medical coverage ends, the subscriber and their dependents covered by this medical plan may be
eligible to continue PEBB medical coverage during temporary or permanent loss of eligibility.
2024 UMP CDHP (PEBB) Certificate of Coverage 153
There are three options the subscriber and their dependents may qualify for when coverage ends.
• PEBB Continuation Coverage (COBRA)
• PEBB Continuation Coverage (Unpaid Leave)
• PEBB retiree insurance coverage
A subscriber also has the right to convert to individual medical insurance coverage with the plan when
continuation of group medical insurance coverage is no longer possible.
PEBB Continuation Coverage
The PEBB Program administers the following continuation coverage options to temporarily extend group
insurance coverage when the enrollee’s PEBB medical plan coverage ends due to a qualifying event:
• PEBB Continuation Coverage (COBRA) includes eligibility and administrative requirements under
federal COBRA laws and regulations. Some enrollees who are not qualified beneficiaries under federal
COBRA, may also qualify for PEBB Continuation Coverage (COBRA).
• PEBB Continuation Coverage (Unpaid Leave) is an option created by the PEBB Program with wider
eligibility criteria and qualifying event types than COBRA.
An enrollee who qualifies for both types of PEBB Continuation Coverage (COBRA and Unpaid Leave) may
enroll in only one of these options. See “Continuation coverage enrollment” and the PEBB Continuation
Coverage Election Notice.
Premium payments for PEBB Continuation Coverage
If a subscriber enrolls in continuation coverage, the subscriber is responsible for timely payment of
premiums and applicable premium surcharges.
PEBB retiree insurance coverage
The following are eligible to continue enrollment or defer enrollment in PEBB retiree insurance coverage if
they meet procedural and substantive eligibility requirements:
• Retiring employee
• Retiring school employee
• Eligible elected or full-time appointed official of the legislative or executive branch of state government
leaving public office
• Dependent becoming eligible as a survivor
• Retiree or survivor enrolled in PEBB retiree insurance coverage
For details, see the PEBB Retiree Enrollment Guide.
Family and Medical Leave Act of 1993
An employee on approved leave under the federal Family and Medical Leave Act (FMLA) may continue to
receive the employer contribution toward PEBB benefits in accordance with the federal FMLA.
The employing agency determines if the employee is eligible for leave and the duration of the leave under
FMLA. The employee must continue to pay their monthly premium contribution and applicable premium
surcharges during this period to maintain eligibility.
If an employee exhausts the period of leave approved under FMLA, they may continue PEBB insurance
coverage by self-paying the monthly premium and applicable premium surcharges set by HCA, with no
contribution from the employing agency. See “Options for continuing PEBB medical coverage.”
154 2024 UMP CDHP (PEBB) Certificate of Coverage
Paid Family and Medical Leave Act
An employee on approved leave under the Washington State Paid Family and Medical Leave (PFML)
Program may continue to receive the employer contribution toward PEBB benefits.
The Employment Security Department determines if the employee is eligible for leave under PFML. The
employee must continue to pay their monthly premium contribution and applicable premium surcharges
during this period to maintain eligibility.
If an employee exhausts the period of leave approved under PFML, they may continue PEBB insurance
coverage by self-paying the monthly premium and applicable premium surcharges set by HCA, with no
contribution from the employing agency. See “Options for continuing PEBB medical coverage.”
Conversion of coverage
An enrollee (including a spouse or dependent of a subscriber terminated for cause) has the right to switch
from PEBB group medical to an individual conversion plan offered by this plan when they are no longer
eligible to continue the PEBB group medical plan and are not eligible for Medicare or covered under
another group insurance coverage that provides benefits for hospital or medical care.
An enrollee must apply for conversion coverage and pay the first month’s premium no later than 31 days
after their group medical plan ends or within 31 days from the date the notice of termination of coverage
is received, whichever is later.
Evidence of insurability (proof of good health) is not required to obtain the conversion coverage. Rates,
coverage, and eligibility requirements of this conversion plan differ from those of the enrollee’s current
group medical plan. To receive detailed information on conversion options under this medical plan, call us
at 1-888-849-3681 (TRS: 711).
General provisions for eligibility and enrollment
Payment of premiums during a labor dispute
Any employee or dependent whose monthly premiums are paid in full or in part by the employing agency
may pay premiums directly to HCA if the employee’s compensation is suspended or terminated directly or
indirectly because of a strike, lockout, or any other labor dispute, for a period not to exceed six months.
When the employee’s compensation is suspended or terminated, HCA will notify the employee
immediately, by mail at the last address of record, that the employee may pay premiums as they become
due.
If coverage is no longer available to the employee under this certificate of coverage, then the employee
may be eligible to purchase an individual medical plan from this plan consistent with premium rates filed
with the Washington State Office of the Insurance Commissioner.
Termination for just cause
The purpose of this provision is to allow for a fair and consistent method to process the plan-designated
provider’s request to terminate coverage from this plan for just cause.
An eligible dependent may have coverage terminated by HCA for the following reasons:
• Failure to comply with the PEBB Program’s procedural requirements, including failure to provide
information or documentation requested by the due date in written requests from the PEBB Program
• Knowingly providing false information
• Failure to pay the monthly premium and applicable premium surcharges when due
• Misconduct. Examples of such termination include, but are not limited to the following:
2024 UMP CDHP (PEBB) Certificate of Coverage 155
▪ Fraud, intentional misrepresentation or withholding of information the subscriber knew or should
have known was material or necessary to accurately determine eligibility or the correct premium
▪ Abusive or threatening conduct repeatedly directed to an HCA employee, a health plan, or other
HCA-contracted vendor providing PEBB insurance coverage on behalf of HCA, its employees, or
other persons
The PEBB Program will enroll an employee and their eligible dependents in another PEBB medical plan
upon termination from this plan.
Appeal rights
Any current or former employee of a state agency or their dependent may appeal a decision made by
the state agency regarding PEBB eligibility, enrollment, or premium surcharges to the state agency.
Any current or former employee of an employer group, such as a county, city, port, water district, etc.,
that contracts with HCA for PEBB benefits, or their dependent may appeal a decision made by an
employer group regarding PEBB eligibility, enrollment, or premium surcharges to the employer group.
Any enrollee may appeal a decision made by the PEBB Program regarding PEBB eligibility, enrollment,
premium payments, or premium surcharges to the PEBB Appeals Unit.
Any enrollee may appeal a decision regarding the administration of a PEBB medical plan by following the
appeal provisions of the plan, except when regarding eligibility, enrollment, and premium payment
decisions.
Learn more at hca.wa.gov/pebb-appeals.
Relationship to law and regulations
Any provision of this certificate of coverage that is in conflict with any governing law or regulation of
Washington State is hereby amended to comply with the minimum requirements of such law or
regulation.
Eligibility and enrollment for a retiree or
survivor
In these sections, the term “retiree” or “retiring employee” includes a retiring employee from a Public
Employees Benefits Board (PEBB) employing agency or employer group, and an elected or full-time
appointed official of the legislative and executive branch of state government eligible to continue
enrollment in PEBB retiree insurance coverage. The term “retiree” or “retiring school employee” includes a
retiring school employee from a School Employees Benefits Board (SEBB) organization or employer group.
Additionally, “health plan” is used to refer to a plan offering medical or dental, or both, developed by
PEBB and provided by a contracted vendor or self-insured plans administered by the Health Care
Authority (HCA).
Eligibility for subscribers and dependents
Retiree eligibility
The PEBB Program determines if a retiring employee or retiring school employee is eligible to enroll in
PEBB retiree insurance coverage upon receipt of their election to enroll. If the retiring employee or retiring
school employee does not have substantive eligibility or does not meet the procedural requirements for
enrollment in PEBB retiree insurance coverage, the PEBB Program will notify them of their right to appeal
eligibility decisions. Information about appeals can be found under “Appeal rights.”
156 2024 UMP CDHP (PEBB) Certificate of Coverage
Survivor eligibility
The PEBB Program determines whether a dependent is eligible to enroll or continue enrollment in PEBB
retiree insurance coverage as a survivor upon receipt of their election to enroll. If the survivor does not
meet the eligibility and procedural requirements for enrollment in PEBB retiree insurance coverage, the
PEBB Program will notify them of their right to appeal. Information about appeals can be found under
“Appeal rights.”
Dependent eligibility
The following are eligible dependents:
• Legal spouse
• State-registered domestic partner and substantially equivalent legal unions from jurisdictions as
defined in Washington State statute. Individuals in a state-registered domestic partnership are treated
the same as a legal spouse except when in conflict with federal law.
• Children, through the last day of the month in which their 26th birthday occurred regardless of marital
status, student status, or eligibility for coverage under another plan. It also includes children age 26 or
older with a disability as described below in “Children of any age with a developmental or physical
disability.” Children are defined as the subscriber’s:
▪ Children based on establishment of a parent-child relationship, as described in Washington
State statutes, except when parental rights have been terminated.
▪ Children of the subscriber’s spouse, based on the spouse’s establishment of a parent-child
relationship, except when parental rights have been terminated. The stepchild’s relationship to the
subscriber (and eligibility as a dependent) ends on the same date the marriage with the spouse ends
through divorce, annulment, dissolution, termination, or death.
▪ Children for whom the subscriber has assumed a legal obligation for total or partial support in
anticipation of adoption of the child.
▪ Children of the subscriber’s state-registered domestic partner, based on the state-registered
domestic partner’s establishment of a parent-child relationship, except when parental rights have
been terminated. The child’s relationship to the subscriber (and eligibility as a dependent) ends on
the same date the subscriber’s legal relationship with the state-registered domestic partner ends
through divorce, annulment, dissolution, termination, or death.
▪ Children specified in a court order or divorce decree for whom the subscriber has a legal
obligation to provide support or health care coverage.
▪ Extended dependents in the legal custody or legal guardianship of the subscriber, the
subscriber’s spouse, or the subscriber’s state-registered domestic partner. The legal
responsibility is demonstrated by a valid court order and the child’s official residence with the
custodian or guardian. Extended dependent child does not include foster children unless the
subscriber, the subscriber’s spouse, or the subscriber’s state-registered domestic partner has
assumed a legal obligation for total or partial support in anticipation of adoption.
▪ Children of any age with a developmental or physical disability that renders them incapable of
self-sustaining employment and chiefly dependent upon the subscriber for support and
maintenance, provided such condition occurs before the age of 26. The following requirements
apply to a dependent child with a disability:
◦ The subscriber must provide proof of the disability and dependency within 60 days of the child’s
attainment of age 26.
2024 UMP CDHP (PEBB) Certificate of Coverage 157
◦ The subscriber must notify the PEBB Program in writing when the child is no longer eligible under
this subsection.
◦ A child with a developmental or physical disability who becomes self-supporting is not eligible as
of the last day of the month in which they become capable of self-support.
◦ A child with a developmental or physical disability age 26 and older who becomes capable of self-
support does not regain eligibility if they later become incapable of self-support.
◦ The PEBB Program, with input from the medical plan, will periodically verify the eligibility of a
dependent child with a disability beginning at age 26, but no more frequently than annually after
the two-year period following the child’s 26th birthday. Verification will require renewed proof of
disability and dependence from the subscriber.
A retiree, a survivor, or their enrolled dependents are required to enroll in Medicare Part A and
Part B if eligible. Any enrollee who is eligible for Medicare must enroll and stay enrolled in Medicare Part
A and Part B to enroll in or continue enrollment in a PEBB retiree health plan. A subscriber must provide a
copy of their or their dependent’s Medicare card or entitlement letter from the Social Security
Administration with Medicare Part A and Part B effective dates to the PEBB Program as proof of Medicare
enrollment. If a subscriber or their dependent is not enrolled in either Medicare Part A or Part B on their
65th birthday, the subscriber must provide the PEBB Program with a copy of the denial letter from the
Social Security Administration. The only exception to this rule is for an employee or school employee who
retired on or before July 1, 1991.
Enrollment for subscribers and dependents
Deferring enrollment
A retiring employee, a retiring school employee, or a dependent becoming eligible as a survivor may
defer (postpone) enrollment in PEBB retiree insurance coverage if they meet the substantive eligibility
requirements to enroll and also meet the procedural requirement by electing to defer enrollment using
Benefits 24/7, the online enrollment system (once available), or by submitting a PEBB Retiree Election Form
(form A) to the PEBB Program within the enrollment timelines.
Deferring enrollment in PEBB retiree insurance coverage will also defer enrollment for all eligible
dependents, except as described below.
A retiring employee, a retiring school employee, or a dependent becoming eligible as a survivor who does
not enroll in PEBB retiree insurance coverage is only eligible to enroll later if they have deferred
enrollment for one or more of the qualifying coverages below:
• Beginning January 1, 2001, enrollment in PEBB retiree insurance coverage may be deferred when the
subscriber is enrolled in employer-based group medical insurance as an employee or the dependent of
an employee, or such medical insurance continued under Consolidated Omnibus Budget Reconciliation
Act (COBRA) coverage or continuation coverage.
• Beginning January 1, 2001, enrollment in PEBB retiree insurance coverage may be deferred when the
subscriber is enrolled as a retiree or the dependent of a retiree in a federal retiree medical plan.
• Beginning January 1, 2006, enrollment in PEBB retiree insurance coverage may be deferred when the
subscriber is enrolled in Medicare Parts A and B and a Medicaid program that provides creditable
coverage. Eligible dependents who are not enrolled in Medicaid coverage that provides creditable
coverage may be enrolled.
• Beginning January 1, 2014, subscribers who are not eligible for Medicare Part A and Part B may defer
enrollment in PEBB retiree insurance coverage when the subscriber is enrolled in qualified health plan
coverage through a health benefit exchange developed under the Affordable Care Act.
158 2024 UMP CDHP (PEBB) Certificate of Coverage
• Beginning July 17, 2018, enrollment in PEBB retiree insurance coverage may be deferred when the
subscriber is enrolled in the Civilian Health and Medical Program of the Department of Veterans Affairs
(CHAMPVA).
Exception: A retiree may defer enrollment in PEBB retiree insurance coverage during the period of time
they are enrolled as a dependent in a medical plan sponsored by PEBB or School Employees Benefits
Board (SEBB), including such coverage under COBRA or continuation coverage. They do not need to elect
to defer enrollment online or submit a PEBB Retiree Election Form.
If a retiree or a survivor chooses to defer enrollment in PEBB medical, enrollment in PEBB dental will also
be deferred.
Enrollment in PEBB retiree insurance coverage is automatically deferred if a retiree or a survivor becomes
eligible for the employer contribution toward PEBB benefits. They do not need to elect to defer
enrollment online or submit a PEBB Retiree Election Form.
If a retiree or a survivor becomes eligible for the employer contribution toward SEBB benefits and enrolls
in a SEBB health plan, they may request to defer enrollment in PEBB retiree insurance coverage.
A retiree or a survivor who deferred their enrollment in PEBB retiree insurance coverage may enroll as
described in the section titled “Enrollment following deferral.”
Retiree and survivor enrollment
An eligible retiree, a survivor, or their dependent can enroll in only one PEBB medical plan, even if
eligibility criteria is met under two or more subscribers.
An eligible retiring employee or a retiring school employee must enroll using Benefits 24/7, the online
enrollment system (once available), or submit a PEBB Retiree Election Form (form A) along with any other
required forms and supporting documents to the PEBB Program. The online enrollment must be
completed or the forms must be received no later than 60 days after the employee’s or the school
employee’s own employer-paid coverage, COBRA coverage, or continuation coverage ends. The first
premium payment and applicable premium surcharges are due to HCA no later than 45 days after the
election period ends.
An eligible elected or full-time appointed official must enroll using Benefits 24/7, the online
enrollment system (once available), or submit a PEBB Retiree Election Form (form A) along with any other
required forms and supporting documents to the PEBB Program. The online enrollment must be
completed or the forms must be received no later than 60 days after the official leaves public office. The
first premium payment and applicable premium surcharges are due to HCA no later than 45 days after the
election period ends.
An eligible survivor of a retiree must submit a PEBB Retiree Election Form (form A) along with any other
required forms and supporting documents to the PEBB Program. They must be received no later than 60
days after the death of the retiree.
An eligible survivor of an employee or school employee must submit a PEBB Retiree Election Form
(form A) along with any other required forms and supporting documents to the PEBB Program. They must
be received no later than 60 days after the later of the date of the employee’s or the school employee’s
death, or the date the survivor’s PEBB insurance coverage, educational service district coverage, or SEBB
insurance coverage ends. The first premium payment and applicable premium surcharges are due to HCA
no later than 45 days after the election period ends.
An eligible employee or school employee determined to be retroactively eligible for disability
retirement must enroll using Benefits 24/7, the online enrollment system (once available), or submit a
PEBB Retiree Election Form (form A) along with any other required forms, supporting documents, and their
formal determination letter to the PEBB Program. The online enrollment must be completed or the forms
2024 UMP CDHP (PEBB) Certificate of Coverage 159
must be received no later than 60 days after the date on the determination letter. The first premium
payment and applicable premium surcharges are due to HCA no later than 45 days after the election
period ends.
An eligible survivor of an emergency service personnel killed in the line of duty must submit a PEBB
Retiree Election Form (form A) along with any other required forms and supporting documents to the PEBB
Program. They must be received no later than 180 days after the later of:
• The date on the letter from the Department of Retirement Systems or the Board for Volunteer
Firefighters and Reserve Officers that informs the survivor that they are determined to be an eligible
survivor;
• The date of the emergency service worker’s death; or
• The last day the survivor was covered under any health plan through the emergency service worker’s
employer or COBRA coverage from the emergency service worker’s employer.
A retiree or a survivor who deferred enrollment and is enrolling in a PEBB retiree health plan, must
enroll using Benefits 24/7, the online enrollment system (once available), or submit a PEBB Retiree Election
Form (form A) along with any other required forms, supporting documents, and evidence of continuous
enrollment to the PEBB Program. The online enrollment must be completed or the forms must be received
no later than 60 days after a loss of other qualifying coverage. The first premium payment and applicable
premium surcharges are due to HCA no later than 45 days after the election period ends. See “Enrollment
following deferral” for additional enrollment timelines.
Note: Enrollment in the PEBB Program’s Medicare Advantage Prescription Drug (MAPD) plan may not be
retroactive. If a subscriber elects an MAPD plan and the online enrollment or the required forms are
received by the PEBB Program after the date PEBB retiree insurance coverage is to begin, the subscriber
and their enrolled dependents will be enrolled in the Uniform Medical Plan Classic during the gap
month(s) prior to when the MAPD plan begins.
Dependent enrollment
To enroll an eligible dependent, the subscriber must include the dependent’s information online using
Benefits 24/7 (once available) or on the applicable enrollment form and provide the required document(s)
as proof of the dependent’s eligibility. The dependent will not be enrolled in PEBB health plan coverage if
the PEBB Program is unable to verify their eligibility within the PEBB Program enrollment timelines.
Dependents who are enrolled in medical coverage must be enrolled in the same PEBB medical plan as the
retiree or survivor.
Exception: If a retiree or a survivor selects a Medicare Supplement Plan or a Medicare Advantage
Prescription Drug plan, non-Medicare enrollees will be enrolled in the Uniform Medical Plan Classic.
A retiree or a survivor may also enroll an eligible dependent during the PEBB Program’s annual open
enrollment or during a special open enrollment. See “Making changes.”
Medicare eligibility and enrollment
Medicare Part A and Part B
If a subscriber or their enrolled dependent becomes eligible for Medicare, they should contact the
Social Security Administration to ask about Medicare enrollment.
Any enrollee who is eligible for Medicare must enroll and stay enrolled in Medicare Part A and Part
B to continue enrollment in a PEBB retiree health plan.
In most cases, Medicare will become the primary insurance coverage and the PEBB retiree medical plan
will become the secondary insurance coverage.
160 2024 UMP CDHP (PEBB) Certificate of Coverage
A subscriber must provide a copy of their or their dependent’s Medicare card or entitlement letter from
the Social Security Administration with effective dates by uploading it online using Benefits 24/7 (once
available) or providing it to the PEBB Program. If a subscriber or their dependent is not enrolled in either
Medicare Part A or Part B on their 65th birthday, the subscriber must upload or provide a copy of the
denial letter from the Social Security Administration. If this procedural requirement is not met, eligibility
will end as described in the termination notice sent by the PEBB Program. The only exception to this rule
is for an employee or school employee who retired on or before July 1, 1991.
Medicare Part D
The PEBB Program has determined that this medical plan has prescription drug coverage that is, on
average, as good as or better than the standard Medicare Part D prescription drug coverage (it is
“creditable coverage”). Therefore, a subscriber or their enrolled dependent cannot enroll in a Medicare
Part D plan and stay in this medical plan.
If the subscriber terminates this medical plan, they may contact the PEBB Program to request a certificate
of creditable coverage. If creditable prescription drug coverage is not maintained, Medicare Part D
premiums may be higher in the future.
If a subscriber, or their enrolled dependent chooses to enroll in a Medicare Part D plan, PEBB retiree
insurance coverage may only be continued by enrolling in the PEBB-sponsored Medicare supplement
plan.
When medical coverage begins
For an eligible retiring employee or retiring school employee and their eligible dependents, medical
coverage begins the first day of the month after the retiring employee’s or retiring school employee’s own
employer-paid coverage, COBRA coverage, or continuation coverage ends.
For an eligible employee or school employee determined to be retroactively eligible for disability
retirement and their eligible dependents, medical coverage begins on the date chosen by the employee
or school employee as allowed under PEBB Program rules.
For an eligible elected or full-time appointed official and their eligible dependents, medical coverage
begins the first day of the month following the date the official leaves public office.
For an eligible survivor of a retiree and their eligible dependents, medical coverage will be continued
without a gap, subject to payment of premiums and applicable premium surcharges. If the eligible
survivor is not enrolled at the time of the retiree’s death, medical coverage will begin the first day of the
month following the retiree’s death.
For an eligible survivor of an employee or school employee and their eligible dependents, medical
coverage begins the first day of the month following the later of the date of the employee’s or the school
employee’s death or the date the survivor’s PEBB insurance coverage, educational service district
coverage, or SEBB insurance coverage ends. This does not include emergency service personnel killed in
the line of duty.
For an eligible survivor of an emergency service personnel killed in the line of duty and their eligible
dependents, medical coverage begins on the date chosen, as allowed under PEBB Program rules.
For a retiree or a survivor who deferred enrollment and is enrolling in a PEBB retiree health plan
following loss of other qualifying coverage, medical coverage for the retiree or the survivor and their
eligible dependents begins the first day of the month after the loss of the other qualifying coverage.
For a retiree, a survivor, or their eligible dependents enrolling during the PEBB Program’s annual
open enrollment, medical coverage begins January 1 of the following year.
2024 UMP CDHP (PEBB) Certificate of Coverage 161
For a retiree, a survivor, or their eligible dependents enrolling during a special open enrollment,
medical coverage begins the first of the month following the later of the event date or the date the online
enrollment election using Benefits 24/7 (once available) or the required form is received. If that day is the
first of the month, medical coverage begins on that day, except for a Medicare Advantage or Medicare
Advantage Prescription Drug plan, which will begin the first day of the month following the date the
enrollment election is received online or the required from is received by the PEBB Program.
If the special open enrollment is due to the birth or adoption of a child, or when the subscriber has
assumed a legal obligation for total or partial support in anticipation of adoption of a child, medical
coverage will begin as follows:
• For a newly born child, medical coverage will begin the date of birth;
• For a newly adopted child, medical coverage will begin on the date of placement or the date a legal
obligation is assumed in anticipation of adoption, whichever is earlier; or
• For a spouse or state registered domestic partner of a subscriber, medical coverage will begin the
first day of the month in which the event occurs.
If the special open enrollment is due to the enrollment of an extended dependent or a dependent child
with a disability, medical coverage will begin the first day of the month following the later of the event
date or eligibility certification, whichever is later.
Making changes
Removing a dependent who is no longer eligible
A subscriber must provide notice to remove a dependent who is no longer eligible due to divorce,
annulment, dissolution, or a qualifying event of a dependent ceasing to be eligible as a dependent child,
as described under “Dependent eligibility.” The notice must be received online using Benefits 24/7 (once
available) or by written request to the PEBB Program within 60 days of the last day of the month the
dependent no longer meets the eligibility criteria.
Consequences for not submitting notice within the required 60 days may include, but are not limited to:
• The dependent may lose eligibility to continue PEBB medical coverage under one of the continuation
coverage options described in “Options for continuing PEBB medical coverage.”
• The subscriber may be billed for claims paid by the medical plan for services that were rendered after
the dependent lost eligibility.
• The subscriber may not be able to recover subscriber-paid insurance premiums for the dependent that
lost eligibility.
• The subscriber may be responsible for premiums paid by the state for the dependent’s medical plan
coverage after the dependent lost eligibility.
Voluntary termination
An enrolled retiree or survivor may voluntarily terminate enrollment in a medical plan at any time by
submitting a request online using Benefits 24/7 (once available) or in writing to the PEBB Program.
Enrollment in the medical plan will be terminated the last day of the month in which the request is
received online or by the PEBB Program, or on the last day of the month specified in the termination
request, whichever is later. If the request is received on the first day of the month, medical plan
enrollment will be terminated on the last day of the previous month. When a retiree, a survivor, or their
dependent is enrolled in a Medicare Advantage or Medicare Advantage Prescription Drug plan, medical
plan enrollment will be terminated on the last day of the month when the PEBB Medicare Advantage Plan
Disenrollment Form (form D) is received.
162 2024 UMP CDHP (PEBB) Certificate of Coverage
A retiree or a survivor who voluntarily terminates their enrollment in a medical plan also terminates all
other health plan enrollment and enrollment for all eligible dependents. Once coverage is terminated, a
retiree or a survivor may not enroll again in the future unless they reestablish eligibility for PEBB insurance
coverage by becoming newly eligible.
Deferring enrollment
An enrolled retiree or survivor may defer enrollment in PEBB retiree insurance coverage at any time by
submitting the request online using Benefits 24/7 (once available) or the PEBB Retiree Change Form (form
E) along with any other required forms and supporting documents to the PEBB Program. Enrollment in
PEBB retiree insurance coverage will be deferred effective the first of the month following the date the
request is received online or by the PEBB Program. If the request is received on the first day of the month,
enrollment will be deferred effective that day. When a retiree, a survivor, or their dependent is enrolled in
a Medicare Advantage or Medicare Advantage Prescription Drug plan, medical plan enrollment will be
deferred the first of the month following the date the PEBB Medicare Advantage Plan Disenrollment Form
(form D) is received. A retiree or a survivor who deferred their enrollment may enroll as described in
“Enrollment following deferral.”
Enrollment following deferral
A retiree or a survivor who defers enrollment in PEBB retiree insurance coverage:
• While enrolled in employer-based group medical or such coverage under COBRA coverage or
continuation coverage may enroll in a PEBB medical plan during the PEBB Program’s annual open
enrollment period, or no later than 60 days after the date their enrollment in employer-based group
medical coverage or such coverage under COBRA coverage or continuation coverage ends.
• While enrolled in a federal retiree medical plan as a retiree or dependent will have a one-time
opportunity to enroll in a PEBB medical plan during the PEBB Program’s annual open enrollment
period, or no later than 60 days after their enrollment in a federal retiree medical plan ends.
• While enrolled in Medicare Parts A and B and a Medicaid program that provides creditable
coverage may enroll in a PEBB medical plan during the PEBB Program’s annual open enrollment
period, or no later than 60 days after their Medicaid coverage ends, or no later than the end of the
calendar year when their Medicaid coverage ends if they were also enrolled in a subsidized Medicare
Part D plan.
• While enrolled in qualified health plan coverage through a health benefit exchange developed
under the Affordable Care Act will have a one-time opportunity to enroll or reenroll in a PEBB medical
plan during the PEBB Program’s annual open enrollment period, or no later than 60 days after
exchange coverage ends.
• While enrolled in CHAMPVA will have a one-time opportunity to enroll in a PEBB medical plan during
the PEBB Program’s annual open enrollment period, or no later than 60 days after their enrollment in a
CHAMPVA medical plan ends.
• While enrolled as a dependent in a medical plan sponsored by PEBB or SEBB, including coverage
under COBRA or continuation coverage, may enroll in a PEBB medical plan during the PEBB Program’s
annual open enrollment period, or no later than 60 days after the enrollment in a medical plan
sponsored by PEBB or SEBB ends, or such coverage under COBRA or continuation coverage ends. The
evidence of continuous enrollment required to enroll as described below may include a health plan
sponsored by a Washington State educational service district if enrollment was deferred prior to
January 1, 2024.
Note: Enrollment in the PEBB Program’s Medicare Advantage Prescription Drug (MAPD) plan may not be
retroactive. If a subscriber elects an MAPD plan and the online enrollment or the required forms are
received by the PEBB Program after the date PEBB retiree insurance coverage is to begin, the subscriber
2024 UMP CDHP (PEBB) Certificate of Coverage 163
and their enrolled dependents will be enrolled in the Uniform Medical Plan Classic during the gap
month(s) prior to when the MAPD plan begins.
For a retiree or a survivor to enroll in a PEBB medical plan, the enrollment must be completed online using
Benefits 24/7 (once available) or the PEBB Program must receive a PEBB Retiree Election Form (form A), any
other required forms, supporting documents, and evidence of continuous enrollment in one or more
qualifying coverages during the timelines described in this section. A gap in coverage of 31 days or less is
allowed between the date PEBB retiree insurance coverage is deferred and the start date of a qualifying
coverage, and between each period of enrollment in qualifying coverages during the deferral period.
A retiree or a survivor who deferred their enrollment in PEBB retiree insurance coverage while enrolled in
qualifying coverage as described above may also enroll in a PEBB medical plan if they receive formal
notice that HCA has determined it is more cost-effective to enroll in a PEBB medical plan than a medical
assistance program.
A retiree or a survivor should contact the PEBB Program or visit hca.wa.gov/pebb-retirees to get the
required forms, information on premiums, and a list of available medical plans.
Making changes during annual open enrollment and special
open enrollment
A subscriber may make certain changes to their enrollment during the annual open enrollment and if a
specific life event creates a special open enrollment period.
Annual open enrollment changes
A subscriber may make the following changes to their enrollment during the PEBB Program’s annual open
enrollment period:
• Enroll in a medical plan following a deferral
• Defer or terminate their enrollment in a medical plan
• Enroll or remove eligible dependents
• Change their medical plan
A subscriber must submit the election change online using PEBB My Account or Benefits 24/7 (once
available) or submit the required PEBB Retiree Election Form (form A-OE) along with any other required
forms, and any supporting documents to the PEBB Program. The change must be completed online or the
forms must be received no later than the last day of the annual open enrollment period and will be
effective January 1 of the following year.
Special open enrollment changes
A subscriber may change their enrollment outside of the annual open enrollment period if a qualifying
event creates a special open enrollment period. However, the change in enrollment must be allowable
under Internal Revenue Code (IRC) and Treasury Regulations and correspond to and be consistent with
the event that creates the special open enrollment for the subscriber, their dependent, or both.
The subscriber must provide evidence of the event that created the special open enrollment.
To disenroll from a Medicare Advantage (MA) plan or Medicare Advantage Prescription Drug (MAPD)
plan, the change in enrollment must be allowable under federal regulations.
To make an enrollment change, the subscriber must submit the change online using Benefits 24/7 (once
available) or submit the required PEBB Retiree Change Form (form E) along with any other required forms
to the PEBB Program. The change must be completed online or the PEBB Program must receive the forms
no later than 60 days after the event that creates the special open enrollment. In addition, the PEBB
164 2024 UMP CDHP (PEBB) Certificate of Coverage
Program will require the subscriber to provide proof of the dependent’s eligibility, evidence of the event
that created the special open enrollment, or both.
Exceptions:
• A subscriber enrolled in PEBB retiree insurance coverage has six months from the date of their or their
dependent’s enrollment in Medicare Part B to change their enrollment to a PEBB Medicare Supplement
Plan. The change must be made online or the PEBB Program must receive the required form(s) no later
than six months after the enrollment in Medicare Part B for either the subscriber or their dependent.
• When a subscriber or their dependent is enrolled in an MA or MAPD plan, they may disenroll during a
special enrollment period as allowed under federal regulations. The new medical plan coverage will
begin the first day of the month following the date the PEBB Medicare Advantage Plan Disenrollment
Form (form D) is received.
• A subscriber enrolled in PEBB retiree insurance coverage has seven months to enroll in an MA or MAPD
plan that begins three months before they or their dependent first enrolled in both Medicare Part A
and Part B and ends three months after the month of Medicare eligibility. A subscriber may also enroll
themselves or their dependent in an MA or MAPD plan before their last day of the Medicare Part B
initial enrollment period. The change must be made online or the forms must be received by the PEBB
Program no later than the last day of the month prior to the month the subscriber or their dependent
enrolls in the MA or MAPD plan.
• If a subscriber wants to enroll a newborn or child whom the subscriber has adopted or has assumed a
legal obligation for total or partial support in anticipation of adoption, the subscriber should complete
the request online or notify the PEBB Program by submitting the required form(s) as soon as possible
to ensure timely payment of claims. If adding the child increases the premium, the request must be
received online, or the required form(s) must be received no later than 60 days after the date of the
birth, adoption, or the date the legal obligation is assumed for total or partial support in anticipation of
adoption.
Special open enrollment events that allow for a change in health plans
A subscriber may not change their health plan during a special open enrollment if their state-registered
domestic partner or state-registered domestic partner’s child is not a tax dependent.
Any of the following events may create a special open enrollment:
• Subscriber gains a new dependent due to:
o Marriage or registering a state-registered domestic partnership.
o Birth, adoption, or assuming a legal obligation for total or partial support in anticipation of adoption.
o A child becoming eligible as an extended dependent through legal custody or legal guardianship.
• Subscriber or their dependent loses other coverage under a group health plan or through health
insurance coverage, as defined by the Health Insurance Portability and Accountability Act (HIPAA).
• Subscriber has a change in employment status that affects their eligibility for the employer contribution
toward their employer-based group health plan.
• Subscriber’s dependent has a change in their own employment status that affects their eligibility or
their dependent’s eligibility for the employer contribution under their employer-based group health
plan. “Employer contribution” means contributions made by the dependent’s current or former
employer toward health coverage as described in the Treasury Regulation.
• Subscriber or their dependent has a change in residence that affects health plan availability. If the
subscriber has a change in residence and their current medical plan is no longer available, the
subscriber must select a new medical plan, as described in PEBB Program rules. If the subscriber does
2024 UMP CDHP (PEBB) Certificate of Coverage 165
not elect a new medical plan as required, they will be enrolled in a PEBB medical plan designated by
the director of HCA or their designee.
• A court order requires the subscriber or any other individual to provide insurance coverage for an
eligible dependent of the subscriber (a former spouse or former state-registered domestic partner is
not an eligible dependent).
• Subscriber or their dependent enrolls in coverage under Medicaid or a state Children’s Health
Insurance Program (CHIP), or the subscriber or their dependent loses eligibility for coverage under
Medicaid or CHIP.
• Subscriber or their dependent becomes eligible for state premium assistance subsidy for PEBB health
plan coverage from Medicaid or CHIP.
• Subscriber or their dependent enrolls in coverage under Medicare, or the subscriber or their dependent
loses eligibility for coverage under Medicare or enrolls in or terminates enrollment in a Medicare
Advantage Prescription Drug or a Part D plan. If the subscriber’s current medical plan becomes
unavailable due to the subscriber or their dependents enrollment in Medicare, the subscriber must
select a new medical plan.
• Subscriber or their dependent’s current medical plan becomes unavailable because the subscriber or
enrolled dependent is no longer eligible for a health savings account (HSA).
• Subscriber or their dependent experiences a disruption of care for active and ongoing treatment that
could function as a reduction in benefits for the subscriber or their dependent. The subscriber may not
change their health plan election because the subscriber or dependent’s physician stops participation
with the subscriber’s health plan unless the PEBB Program determines that a continuity of care issue
exists. The PEBB Program will consider but not limit its consideration to the following:
▪ Active cancer treatment, such as chemotherapy or radiation therapy
▪ Treatment following a recent organ transplant
▪ A scheduled surgery
▪ Recent major surgery still within the postoperative period
▪ Treatment for a high-risk pregnancy
▪ The PEBB Program determines that there has been a substantial decrease in the providers available
under a PEBB medical plan.
Note: The plan cannot guarantee that any physician, hospital, or other provider will be available or remain
under contract with the plan. An enrollee may not change medical plans simply because their provider or
health care facility discontinues participation with this medical plan until the PEBB Program’s next annual
open enrollment or when another qualifying event creates a special open enrollment for changing health
plans, unless the PEBB Program determines that a continuity of care issue exists or there has been a
substantial decrease in the providers available under the plan.
Special open enrollment events that allow adding or removing a dependent
Any of the following events may create a special open enrollment:
• Subscriber gains a new dependent due to:
▪ Marriage or registering a state-registered domestic partnership.
▪ Birth, adoption, or when the subscriber has assumed a legal obligation for total or partial support in
anticipation of adoption.
▪ A child becoming eligible as an extended dependent through legal custody or legal guardianship.
166 2024 UMP CDHP (PEBB) Certificate of Coverage
• Subscriber or their dependent loses other coverage under a group health plan or through health
insurance coverage, as defined by the Health Insurance Portability and Accountability Act (HIPAA).
• Subscriber has a change in employment status that affects their eligibility for the employer contribution
toward their employer-based group health plan.
• Subscriber’s dependent has a change in their own employment status that affects their eligibility or
their dependent’s eligibility for the employer contribution under their employer-based group health
plan. “Employer contribution” means contributions made by the dependent’s current or former
employer toward health coverage as described in the Treasury Regulation.
• Subscriber or their dependent has a change in enrollment under an employer-based group health plan
during its annual open enrollment that does not align with the PEBB Program’s annual open
enrollment.
• Subscriber’s dependent has a change in residence from outside of the United States to within the
United States, or from within the United States to outside of the United States and that change in
residence resulted in the dependent losing their health insurance.
• A court order requires the subscriber or any other individual to provide insurance coverage for an
eligible dependent of the subscriber (a former spouse or former state-registered domestic partner is
not an eligible dependent).
• Subscriber or their dependent enrolls in coverage under Medicaid or a state Children’s Health
Insurance Program (CHIP) or the subscriber or their dependent loses eligibility for coverage under
Medicaid or CHIP.
• Subscriber or their dependent becomes eligible for a state premium assistance subsidy for PEBB health
plan coverage from Medicaid or CHIP.
• Subscriber’s dependent enrolls in Medicare or loses eligibility for Medicare.
When medical coverage ends
Termination dates
Medical coverage ends on the following dates:
• On the last day of the month when any enrollee ceases to be eligible.
• On the date a medical plan terminates due to a change in contracted service area or when the group
policy ends. If that should occur, the subscriber will have the opportunity to enroll in another PEBB
medical plan.
• On the last day of the month in which the monthly premium and applicable premium surcharges were
paid. When a subscriber is enrolled in a Medicare Advantage (MA) or a Medicare Advantage
Prescription Drug (MAPD) plan, medical coverage ends at the end of the month after a termination
notice is sent. The first of the month following the date the election is received online using Benefits
24/7 (once available) or the required forms are received by the PEBB Program when an enrolled retiree
or survivor requests to defer enrollment in PEBB retiree insurance coverage. If the election is received
on the first day of the month, enrollment will be deferred effective that day. When a retiree, a survivor,
or their dependent is enrolled in an MA or a MAPD plan, medical plan enrollment will be deferred the
first of the month following the date the PEBB Medicare Advantage Plan Disenrollment Form (form D) is
received. The last day of the month in which the request is received online using Benefits 24/7 (once
available) or the PEBB Program receives a written request and all required forms requesting to
voluntarily terminate enrollment in a medical plan. If a future date is specified, medical coverage
terminates the last day of the month specified. If the termination request is received on the first day of
the month, medical plan enrollment will be terminated on the last day of the previous month. When a
2024 UMP CDHP (PEBB) Certificate of Coverage 167
retiree, a survivor, or their dependent is enrolled in an MA or MAPD plan, medical plan enrollment will
be terminated on the last day of the month when the PEBB Medicare Advantage Plan Disenrollment
Form (form D) is received.
A subscriber will be responsible for payment of any services received after the date medical coverage
ends, as described above.
Final premium payments
The subscriber is responsible for timely payment of premiums and applicable premium surcharges.
Premium payments and applicable premium surcharges are not prorated during any month, for any
reason, even if an enrollee dies or asks to terminate their medical plan before the end of the month.
If the monthly premium or applicable premium surcharges remain unpaid for 30 days, it will be
considered delinquent. A subscriber is allowed a grace period of 30 days from the date the monthly
premium or applicable premium surcharges become delinquent to pay the unpaid premium balance or
applicable premium surcharges. If the subscriber’s premium balance or applicable premium surcharges
remain unpaid for 60 days from the original due date, coverage will be terminated retroactive to the last
day of the month for which the monthly premium and any applicable premium surcharges were paid.
For a subscriber enrolled in a Medicare Advantage or Medicare Advantage Prescription Drug plan, a
notice will be sent to them notifying them that they are delinquent on their monthly premiums and that
the enrollment will be terminated prospectively to the end of the month after the notice is sent.
If an enrollee is hospitalized
An enrollee who is receiving covered services in a hospital on the date medical coverage ends will
continue to be eligible for covered services while an inpatient for the condition which the enrollee was
hospitalized, until one of the following events occur:
• According to this plan’s clinical criteria, it is no longer medically necessary for the enrollee to be an
inpatient at the facility.
• The remaining benefits available for the hospitalization are exhausted, regardless of whether a new
calendar year begins.
• The enrollee becomes covered under another agreement with a group health plan that provides
benefits for the hospitalization.
• The enrollee becomes enrolled under an agreement with another carrier that provides benefits for the
hospitalization.
This provision will not apply if the enrollee is covered under another agreement that provides benefits for
the hospitalization at the time medical coverage ends, except as set forth in this section, or if the enrollee
is eligible for PEBB Continuation Coverage as described in “Options for continuing PEBB medical
coverage.”
Options for continuing PEBB medical coverage
A subscriber and their dependents covered by this medical plan may be eligible to continue enrollment
under PEBB Continuation Coverage (COBRA) if they lose eligibility. PEBB Continuation Coverage (COBRA)
temporarily extends group insurance coverage if certain circumstances occur that would otherwise end
the subscriber or their dependent’s PEBB medical coverage. PEBB Continuation Coverage (COBRA)
includes eligibility and administrative requirements under federal COBRA laws and regulations and also
includes coverage for some enrollees who are not qualified beneficiaries under federal COBRA
continuation coverage. Refer to the PEBB Continuation Coverage Election Notice for details.
168 2024 UMP CDHP (PEBB) Certificate of Coverage
A subscriber and their dependents covered by this medical plan who lose eligibility for PEBB retiree
insurance coverage when their employer group ends participation with the Health Care Authority, may be
eligible to continue their enrollment under PEBB Continuation Coverage (Employer Group Ended
Participation).
The PEBB Program administers these coverages. Call the PEBB Program at 1‑800‑200‑1004 (TRS: 711) for
details.
Options for continuing coverage under PEBB Retiree
Insurance Coverage
A dependent becoming eligible as a survivor of a retiree is eligible to continue enrollment or defer
enrollment in PEBB retiree insurance coverage if they meet procedural and substantive eligibility
requirements. See the PEBB Retiree Enrollment Guide for details.
Conversion of coverage
An enrollee (including a spouse or dependent of a subscriber terminated for cause) has the right to switch
from PEBB group medical to an individual conversion plan offered by this plan when they are no longer
eligible to continue the PEBB group medical plan and are not eligible for Medicare or covered under
another group insurance coverage that provides benefits for hospital or medical care.
An enrollee must apply for conversion coverage and pay the first month’s premium no later than 31 days
after their group medical plan ends or within 31 days from the date the notice of termination of coverage
is received, whichever is later.
Evidence of insurability (proof of good health) is not required to obtain the conversion coverage. Rates,
coverage, and eligibility requirements of this conversion plan differ from those of the enrollee’s current
group medical plan. To receive detailed information on conversion options under this medical plan, call us
at 1-888-849-3681 (TRS: 711).
General provisions for eligibility and enrollment
Termination for just cause
The purpose of this provision is to allow for a fair and consistent method to process the plan-designated
provider’s request to terminate an enrollee’s coverage from this plan for just cause.
A retiree or eligible dependent may have coverage terminated by HCA for the following reasons:
• Failure to comply with the PEBB Program’s procedural requirements, including failure to provide
information or documentation requested by the due date in written requests from the PEBB Program
• Knowingly providing false information
• Failure to pay the monthly premium and applicable premium surcharges when due
• Misconduct. Examples of such termination include, but are not limited to the following:
▪ Fraud, intentional misrepresentation or withholding of information the subscriber knew or should
have known was material or necessary to accurately determine eligibility or the correct premium
▪ Abusive or threatening conduct repeatedly directed to an HCA employee, a health plan, or other
HCA-contracted vendor providing PEBB insurance coverage on behalf of HCA, its employees, or
other persons
If a retiree’s PEBB insurance coverage is terminated by HCA for the above reasons, PEBB insurance
coverage for all of the retiree’s eligible dependents is also terminated.
2024 UMP CDHP (PEBB) Certificate of Coverage 169
Appeal rights
Any enrollee may appeal a decision made by the PEBB Program regarding PEBB eligibility, enrollment,
premium payments, or premium surcharges to the PEBB Appeals Unit.
Learn more at hca.wa.gov/pebb-appeals.
Fax: 360-763-4709
Mail: Health Care Authority
Attn: PEBB Appeals Unit
PO Box 45504
Olympia, WA 98504-5504
Hand deliver: Health Care Authority
626 8th Avenue SE
Olympia, WA 98501
Any enrollee may appeal a decision regarding the administration of a PEBB medical plan by following the
appeal provisions of the plan, except when regarding eligibility, enrollment, and premium payment
decisions.
Relationship to law and regulations
Any provision of this certificate of coverage that is in conflict with any governing law or regulation of
Washington State is hereby amended to comply with the minimum requirements of such law or
regulation.
PEBB customer service
For questions about PEBB retiree eligibility and enrollment, call the PEBB Program at 1-800-200-1004
(TRS:711) or visit hca.wa.gov/pebb-retirees.
For questions about Medicare, call the Centers for Medicare and Medicaid Services (CMS) at
1-800-MEDICARE or visit medicare.gov.
Definitions
Allowed amount, medical services
Allowed amount for medical services is the most the plan pays for a specific covered service or supply.
The allowed amount is determined as follows:
• For preferred providers that are within the Regence BlueShield service area, the Preferred Provider
Organization (PPO) contract with Regence BlueShield is the relevant contract that determines the
allowed amount. For preferred providers that are outside the Regence BlueShield service area, the
contract with another Blue Cross or Blue Shield organization in the BlueCard® Program for its PPO
network is the relevant contract that determines the allowed amount.
• For participating providers that are within the Regence BlueShield service area, the participating
provider contract with Regence BlueShield is the relevant contract that determines the allowed amount.
For participating providers that are outside the Regence BlueShield service area, the contract with
another Blue Cross or Blue Shield organization in the BlueCard® Program is the relevant contract that
determines the allowed amount.
170 2024 UMP CDHP (PEBB) Certificate of Coverage
• For out-of-network providers who are within the Regence BlueShield service area and not
contracted with Regence BlueShield, the amount Regence has determined to be reasonable charges
for covered services and supplies is the allowed amount.
The allowed amount may be based upon the billed charges for some services, as determined by
Regence or as otherwise required by law. If a provider is not in the network, as described above, but
has a contract with Regence, the allowed amount is based on the negotiated rate.
• For out-of-network providers accessed through the BlueCard® Program, the allowed amount is
the lower of the provider’s billed charges and the amount that the other Blue plan identifies as the
amount on which it would base a payment to that provider.
Under the BlueCard® Program, when you access covered services within the geographic area served by
a Host Blue, Regence BlueShield will remain responsible for fulfilling contractual obligations. However,
the Host Blue is responsible for contracting with and generally handling all interactions with its network
providers.
Whenever you access covered services outside Regence BlueShield’s service area and the claim is
processed through the BlueCard® Program, the amount you pay for covered services is calculated based
on the lower of:
• The covered billed charges for your covered services; or
• The negotiated price that the Host Blue makes available to Regence.
Often, this negotiated price will be a simple discount that reflects an actual price that the Host Blue pays
to your health care provider. Sometimes, it is an estimated price that considers special arrangements with
your health care provider or provider group that may include types of settlements, incentive payments,
and/or other credits or charges. Occasionally, it may be an average price, based on a discount that results
in expected average savings for similar types of health care providers after considering the same types of
transactions as with an estimated price.
Estimated pricing and average pricing, going forward, also consider adjustments to correct for over- or
underestimation of modifications of past pricing for the types of transaction modifications noted above.
However, such adjustments will not affect the price Regence uses for your claim because they will not be
applied retroactively to claims already paid.
Laws in a small number of states may require the Host Blue to add a surcharge to your calculation. If any
state laws mandate other liability calculation methods, including a surcharge, Regence BlueShield would
then calculate your liability for any covered services according to applicable law.
Charges more than the allowed amount are not reimbursable. For questions regarding the basis for
determination of the allowed amount, contact UMP Customer Service.
Allowed amount, prescription drugs
The allowed amount for prescription drugs is based on WSRxS’ contractually agreed reimbursement,
unless other contractual arrangements or terms apply. All covered prescription drug claims are paid based
on this allowed amount.
Ambulatory surgery center (ASC)
An ambulatory surgery center (ASC) is a health care facility that specializes in providing surgery, pain
management, and certain diagnostic services in an outpatient setting. ASC-qualified procedures are
typically more complex than those done in a doctor’s office but not so complex as to require an overnight
stay. Procedures commonly performed in these centers include colonoscopies, endoscopies, cataract
2024 UMP CDHP (PEBB) Certificate of Coverage 171
surgery, orthopedic, and ENT (ear, nose, and throat) procedures. An ASC may also be known as an
outpatient surgery center or same-day surgery center.
Annual open enrollment
Annual open enrollment is a period of time defined by HCA when a subscriber may change to another
health plan offered by the PEBB Program and make certain other account changes for an effective date
beginning January 1 of the following year.
Appeal
See the “Complaint and appeal procedures” section for an explanation of appeals and how the process
works. For appeals related to PEBB eligibility or enrollment see "Appeal rights" in the "Eligibility and
Enrollment" and in the “Eligibility and enrollment for a retiree or survivor” sections for more information.
Authorized representative
An authorized representative is someone you have designated in writing to communicate with the plan
on your behalf. See page 136 for how this works.
Balance billing
Balance billing is a provider billing you for the difference between the billed amount and the allowed
amount. Preferred and participating providers cannot balance bill you for covered services above the
allowed amount. See an example of how this works in the “Sample payments to different provider
network status” section.
When you receive nonemergency services at a network hospital, network hospital outpatient department,
network critical access hospital, or network ambulatory surgical center in Washington State, you pay the
network rate and cannot be balance billed regardless of the network status of the provider. For
nonemergency services performed at one of these facilities outside of Washington State, you still pay the
network rate, but in some states, an out-of-network provider may be allowed to ask you to waive some of
your balance billing protections.
At an out-of-network facility, when you receive emergency services you cannot be balance billed.
Birthday rule
In some instances, the birthday rule is used to determine which group health plan will pay first for the
dependent children of married, living together and not married, legally separated, or divorced parents.
This rule looks at only the month and day, not the year, of the parents’ birthdays. For example, the plan of
a parent born April 14 is primary over the plan of a parent born August 21. If both parents have the same
birthday, the plan that has covered either parent the longest is primary.
Biosimilar
A biosimilar, or biosimilar drug, is a medicine approved by the US Food and Drug Administration that is
highly similar in structure to and has no clinical difference to a reference biologic medicine.
Brand-name drug
A brand-name drug is a prescription drug sold under the proprietary name or trade name selected by
the manufacturer.
172 2024 UMP CDHP (PEBB) Certificate of Coverage
Business day
Business days are Mondays through Fridays, except for legal holidays observed by Washington State.
Calendar day
A calendar day is any day of the week regardless of whether it is observed as a legal holiday by
Washington State.
Calendar year
A calendar year is January 1 through December 31.
Chronic migraine
A chronic migraine is having a headache on 15 or more days per month of which eight or more days are
a migraine.
Clinical review
Clinical review is when the plan has a clinical professional review medical records related to treatment to
determine if treatment is medically necessary.
Coinsurance
Coinsurance is the percentage of the allowed amount you must pay the provider on claims for which the
plan pays less than 100 percent of the allowed amount. This includes most medical services and
prescription drugs.
Continuation Coverage
Continuation Coverage means the temporary continuation of PEBB benefits available to enrollees under
the Consolidated Omnibus Budget Reconciliation Act (COBRA), the Uniformed Services Employment and
Reemployment Rights Act (USERRA), or PEB Board policies.
Coordination of benefits (COB)
For members covered by more than one group health plan, coordination of benefits (COB) is the
method the plan uses to determine which plan pays first, which pays second, and the amount paid by
each plan. See description and examples in the “If you have other HDHP coverage” section.
Copay
Copay is a set dollar amount you pay when receiving specific services, treatments, or supplies, such as
chiropractic, acupuncture, and massage therapy.
Cost-share
Cost-share means the amount you pay for a service, supply, or prescription drug. This may be a
deductible, coinsurance, or amounts not covered by the plan.
Custodial care
Custodial care is care primarily to assist in activities of daily living, including institutional care primarily to
support self-care and provide room and board. Custodial care includes, but is not limited to, help in
2024 UMP CDHP (PEBB) Certificate of Coverage 173
walking, getting into and out of bed, bathing, dressing, feeding and preparing special diets, and
supervising prescription drugs that are ordinarily self-administered.
Deductible
Your deductible is a fixed dollar amount you must meet each calendar year for your health care expenses
before the plan starts paying for covered services. For this plan, you must meet your deductible for
medical and prescription drug expenses before the plan starts paying for covered medical services and
covered prescription drugs. You pay the first $1,600 in health care expenses for one member enrolled; you
pay the first $3,200 in health care expenses for two or more members enrolled. Only expenses covered by
the plan apply to your deductible. For example, if you receive LASIK surgery (see exclusion on page 108),
the plan does not apply this payment to your deductible. Some services are not subject to this deductible
(see the “Summary of benefits” section). See the “What you pay for services” section for details on how
your deductible works.
Dependent
A dependent is an eligible spouse, state-registered domestic partner, child, or other eligible family
member as described in “Dependent eligibility” (see the “Eligibility for subscribers and dependents”
sections on page 140 and 155) that is either covered by or eligible to be covered by the plan under the
subscriber’s account.
Detoxification
Detoxification is a medically supervised treatment program for individuals with alcohol or drug
intoxication, designed to rid the body of toxic substances and manage withdrawal symptoms.
Developmental delay
Developmental delay is a significant lag in reaching developmental milestones as expected during
infancy and early childhood. The cause may be present at birth or acquired after birth from a disease or
disorder of the body, an injury, a disorder of the mind or emotions, or harmful effects of the surrounding
environment. Only a physician or other provider may diagnose a developmental delay.
Durable medical equipment (DME)
Durable medical equipment (DME) is:
• Designed for prolonged use.
• For a specific therapeutic or clinical purpose, or to assist in the treatment of an injury or illness.
• Medically necessary (meeting all plan medical necessity criteria).
• Primarily and customarily used only for a medical purpose.
See page 108 for examples of equipment that is not covered.
Effectiveness
Effectiveness means the extent to which a specific intervention, procedure, service, level of service,
supply, prescription drug, or drug dose may reasonably be expected to produce the intended results and
to have expected benefits that outweigh potential harmful effects under real-world circumstances.
174 2024 UMP CDHP (PEBB) Certificate of Coverage
Efficacy
Efficacy is the extent to which a specific intervention, procedure, service, supply, or prescription drug
produces the desired effect under ideal conditions (in a controlled environment under lab circumstances).
Elective contact lenses
Elective contact lenses are covered lenses under the frame limit in lieu of coverage for eyeglasses.
Emergency
See the “Medical emergency” definition.
Emergency fill
Emergency fill is a process where the plan covers a limited amount of a prescription drug on an
emergency basis while the plan processes your drug preauthorization request.
Employer group
Employer group for the Public Employees Benefits Board (PEBB) Program means those counties,
municipalities, political subdivisions, the Washington health benefits exchange, tribal governments, and
employee organizations representing state civil service employees obtaining employee benefits through a
contractual agreement with the health care authority (HCA) to participate in benefit plans developed by
the PEB board.
Employer group for the School Employees Benefits Board (SEBB) Program means an employee
organization representing school employees and a tribal school as defined in RCW 28A.715.010, obtaining
employee benefits through a contractual agreement with the health care authority (HCA) to participate in
benefit plans developed by the SEB board.
Employing agency
Employing agency means a division, department, or separate agency of state government, including an
institution of higher education; a county, municipality, or other political subdivision; and a tribal
government covered by chapter 41.05 RCW.
Enrollee
Enrollee means a person who meets all eligibility requirements and is enrolled in PEBB benefits, and for
whom applicable premium payments have been made.
Excluded pharmacy
Excluded pharmacies are pharmacies or pharmacy chains that are prohibited from contracting with the
Pharmacy Network, and that are not eligible to be reimbursed for Prescription Drug Claims. Prescriptions
filled at excluded pharmacies are not covered. Locate a network pharmacy by visiting the UMP
Prescription drug coverage webpage (see Directory for link).
Experimental or investigational
Experimental or investigational means any treatment that is not recognized by the plan as conforming
to standard medical care for the condition, disease, illness, or injury being treated. ”Treatment” in this
setting may include any intervention, therapy, procedure, facility, equipment, drug usage, device, service,
2024 UMP CDHP (PEBB) Certificate of Coverage 175
supply, intervention, biologic product or drug (prescription or nonprescription). Experimental and
investigational treatments are not covered, even if the treatment is considered medically necessary. The
plan will review scientific evidence from well-designed clinical studies found in peer-reviewed medical
literature, if available, and information obtained from the treating provider regarding the treatment to
determine if it is experimental or investigational.
A treatment meeting any of the following criteria is considered experimental or investigational:
• Approval of the treatment or one of its components by one or more government agencies (e.g., FDA) is
required but has not been obtained at the time the treatment is requested or administered.
• The improvement has not been shown to be attainable outside the laboratory or clinical research
setting.
• The scientific evidence does not permit conclusions concerning the effect of the treatment on health
outcomes, which include the disease process, injury or illness, length of life, ability to function, and
quality of life.
• The scientific evidence does not show that the treatment is as beneficial as any established alternatives.
• The treatment has not been demonstrated to improve net health outcomes.
• The treatment has scientific evidence to support its use, but not for the specific indication for which it is
being requested.
• The treatment is a drug or device that is prescribed for other than its FDA-approved use(s) and is not
recognized as “effective” for the use for which it is being prescribed. To be considered “effective” for
other than its FDA-approved use, a prescription drug or device must be so recognized in one of the
standard reference compendia or, if not, then in a majority of relevant peer-reviewed medical literature;
or by the U.S. Secretary of Health and Human Services.
• The treatment is considered to be experimental or investigational by U.S. standards.
• The treatment is drug combination therapy, when the scientific literature only supports the drug’s use
as monotherapy and not when utilized in combination with other drugs.
• The treatment is drug monotherapy, when the scientific literature only supports the drug’s use when
utilized in combination with other drugs.
• The treatment is not provided by a provider that has demonstrated medical proficiency in the provision
of the treatment.
• The treatment is only available in the U.S. as part of a clinical trial or research program for the illness or
condition being treated.
▪ Although the plan does not pay for items, drugs, devices, or services (including items, drugs, devices,
or services provided in a clinical trial) for investigational use, the plan does not deny qualified
individuals from participating in approved clinical trials. The terms “qualified individual” and
“approved clinical trial” are defined in 42 U.S.C. §300gg-8. If a qualified individual is participating in
an approved clinical trial, the plan will not deny, limit, or impose additional conditions on the
coverage for routine patient costs for items and services furnished in connection with participation
in the trial and will not discriminate against the individual on the basis of the individual’s
participation in such trial. The plan will apply its standard terms and conditions for routine patient
costs for items and services furnished in connection with participation in the trial.
• The treatment is the subject of an on-going phase I or phase II clinical trial or is the research,
experimental, study, or investigational arm of an on-going phase III clinical trial.
176 2024 UMP CDHP (PEBB) Certificate of Coverage
Explanation of Benefits (EOB)
An Explanation of Benefits (EOB) is a detailed account of each medical claim processed by the plan,
which the plan sends to you to notify you of claim payment or denial. You may also sign in to your
Regence account or contact UMP Customer Service to request a copy of an EOB (see Directory for link
and contact information). You will need to provide identifying information over the phone.
Family
Family is defined as all eligible family members (subscriber and dependents) who are enrolled on a single
account.
Fee schedule
A fee schedule is a list of the plan’s maximum payment amounts for specific services or supplies.
Preferred providers have agreed to accept these fees as payment in full for services to members. See the
definition of “Allowed amount, medical services” for more details.
Formulary
A formulary is a list available online that specifies how prescription drugs are covered by the plan. By
using this list, you may find out if a prescription drug is covered, if the drug must be ordered through the
plan’s specialty drug pharmacy, and whether the drug has any limitations (such as needing
preauthorization or quantity limits; see the “Limits on your prescription drug coverage” section).
The UMP Preferred Drug List is sometimes called a formulary (see “The UMP Preferred Drug List” section
for more information).
Generic drug
A generic drug is a prescription drug with the same active ingredient(s), but not necessarily the same
inactive ingredients, as a brand-name drug that is no longer protected by a commercial patent. A generic
drug is therapeutically equivalent to the brand-name prescription drug, which means it works like the
brand-name drug in dosage, strength, performance, and use. All generic drugs sold in the U.S. must be
reviewed and approved by the FDA, and meet the same quality and safety standards as brand-name
drugs.
Generic equivalent
A generic equivalent is a generic prescription drug that has the same active ingredients as its brand-
name counterpart. For a generic drug to be considered “equivalent,” it has to be approved by the FDA as
being interchangeable with that brand-name drug. Under Washington State law, the pharmacist is
required to dispense a generic equivalent in place of a brand-name drug, unless your provider objects.
See “Substitution under Washington State Law” on page 100 for how this works.
Gestational Parent
The individual who carries the pregnancy and gives birth.
Grievance
A grievance is also called a complaint. See the “Complaint and appeal procedures” section for details on
how these are handled.
2024 UMP CDHP (PEBB) Certificate of Coverage 177
Habilitative (neurodevelopmental) services
Habilitative (neurodevelopmental) services are health care services that help you keep, learn, or
improve skills and functioning for daily living. Examples include therapy for a child who isn't walking or
talking at the expected age. These services may include physical and occupational therapy, speech-
language pathology, and other services for people with disabilities in a variety of inpatient and/or
outpatient settings.
Health Care Authority (HCA)
The Health Care Authority (HCA) is the Washington State agency that administers the Uniform Medical
Plan (UMP Classic, UMP Select, UMP CDHP, and the UMP Plus plans: UMP Plus–Puget Sound High Value
Network and UMP Plus–UW Medicine Accountable Care Network), in addition to the following health care
programs: Washington Prescription Drug Program, PEBB Program, SEBB Program, Behavioral Health and
Recovery, and Apple Health (also known as Medicaid).
Health intervention
Health intervention is a prescription drug, service, or supply provided to prevent, diagnose, detect, treat,
or palliate the following: disease, illness, injury, genetic or congenital anomaly, pregnancy, or biological or
psychological condition that lies outside the range of normal, age-appropriate human variation. A health
intervention may also maintain or restore functional ability. A health intervention is defined not only by
the intervention itself, but also by the medical condition and patient indications for which it is being
applied. A health intervention is new if it is not yet in widespread use for the medical condition and the
patient indications being considered.
Health outcomes
Health outcomes are results that affect health status as measured by the length or quality (primarily as
perceived by the member) of a person’s life.
Health savings account (HSA)
A health savings account (HSA) is a tax-advantaged spending and savings account that may be used to
pay for qualified medical expenses. IRS rules govern who may have an HSA and how the funds may be
spent. The HSA is funded by pre-tax contributions from you, your employer, or both. See the “Deductibles
and limits” section for information on contribution limits. You may contribute up to the annual limit even
if your health plan deductible is lower. The contribution limits are subject to change every year, adjusted
for inflation.
High-deductible health plan (HDHP)
A high-deductible health plan (HDHP) is any plan with an annual deductible of at least $1,600 for an
individual or $3,200 for a family. UMP CDHP is an HDHP with an HSA.
Home health agency
A home health agency is an agency or organization that:
• Provides a program of home health care;
• Practices within the scope of its license as a provider of home health services; and
• Is Medicare-certified, accredited by the Joint Commission on Accreditation of Healthcare Organizations,
or a preferred provider.
178 2024 UMP CDHP (PEBB) Certificate of Coverage
Hospice
Hospice is services provided by a state-licensed hospice program in the member’s home or in a hospice
facility to terminally ill members. Hospice care includes services such as pain care relief for terminally ill
members without the intent to cure, and support services for their families.
Hospital
A hospital is an institution accredited under the Hospital Accreditation Program of the Joint Commission
and licensed by the state where it is located. A hospital has a defined course of therapeutic intervention
and special programming in a controlled environment. A hospital also offers a degree of security,
supervision, and structure. Hospital patients must be medically monitored with 24-hour medical
availability and 24-hour onsite services as defined in federal guidelines outlining Conditions of
Participation for Hospitals.
The term hospital does not include a convalescent nursing home or institution (or a part of one) that:
• Furnishes primarily domiciliary or custodial care.
• Is operated as a school.
• Is used principally as a convalescent facility, rest facility, nursing facility, or facility for the aged.
Inpatient rate
The inpatient rate means that the plan pays 100 percent of the allowed amount after you pay your
deductible at preferred facilities.
The plan pays for professional services, such as provider visits or lab tests, based on the provider’s
network status during an inpatient stay:
• Preferred providers: You pay 15 percent of the allowed amount after you meet your deductible. The
plan pays 85 percent of the allowed amount.
• Participating providers: You pay 40 percent of the allowed amount after you meet your deductible. The
plan pays 60 percent of the allowed amount.
• Out-of-network providers: You pay 40 percent of the allowed amount after you meet your deductible.
You pay all charges billed to you above the allowed amount (known as balance billing). The plan pays
60 percent of the allowed amount.
Inpatient stay
An inpatient stay begins when you are admitted to a hospital or other medical facility, and ends when
you are discharged from that facility.
Independent review organization (IRO)
An independent review organization (IRO) conducts the independent (or external) review of an appeal.
An IRO is a group of medical and benefit experts certified by the Washington State Department of Health
and not related to the plan, Regence BlueShield, WSRxS, or HCA. An IRO is intended to provide unbiased,
independent clinical and benefit expertise, as well as evidence-based decision making while ensuring
confidentiality. The IRO reviews your appeal to determine if the plan’s decision is consistent with state law
and the applicable COC. The plan pays the IRO’s charges. See “External review (independent review)” on
page 129.

2024 UMP CDHP (PEBB) Certificate of Coverage 179
Intensive Outpatient Program
Intensive Outpatient Program (IOP) is an outpatient program that is licensed as a facility or agency by
the appropriate state agency and is provided under the supervision of a psychiatrist or psychiatric
extender. IOP is intended to provide treatment on an outpatient basis, does not include boarding or
housing, and is intended to provide treatment interventions in a structured setting, with patients returning
to their home environments each day. IOP is a minimum of three hours per day, three days per week.
Limited benefit
TIP: This definition applies only to those benefits in which it is used in this COC. Other benefits
have additional limits related to medical necessity or preauthorization of services (see the
“Limits on plan coverage” section).
A limited benefit is a benefit that is limited to a certain number of visits or a maximum dollar amount.
The limit applies to these benefits even if the provider prescribes additional visits and even if the visits are
medically necessary.
For benefits limited to a certain number of visits, any visits that are applied to your deductible also count
against your annual visit or dollar limit. In addition, visits that are paid by another health plan that is
primary apply to the plan limit. For example, if your primary plan applies your first 12 chiropractor
sessions to your deductible, you may receive coverage for 12 more sessions in that calendar year, for a
total of 24 visits (the visit maximum for chiropractic services). For benefits limited to a certain dollar
amount (e.g., hearing aids), you pay all charges billed to you above the maximum dollar limit. Any
amounts billed above the maximum dollar amount do not apply to your out-of-pocket limit.
These limits apply per member.
Services are counted against a limited benefit according to the type of service, not the provider type.
When a provider practicing within the scope of their license provides services coded under a limited
benefit (e.g., spinal manipulation or physical therapy), those services will be counted against the benefit
regardless of the provider type. In addition, if more than one type of limited benefit service is provided
during a single visit, the services will count against all the limited benefits. For example, if both
manipulation and physical therapy codes are billed for a visit, that visit will count against both the spinal
and extremity manipulation and physical therapy benefit limits.
Maintenance care
Maintenance care is a health intervention after the member has reached maximum rehabilitation
potential or functional level and has shown no significant improvement for one to two weeks, and
instruction in the maintenance program has been completed.
Maintenance care may apply to several different services, including, but not limited to, physical therapy,
speech therapy, neurodevelopmental therapy, home health care, and skilled nursing care.
Medical
Medical generally refers to all plan benefits and services other than those covered under preventive care
and prescription drug benefits (except as the term is used in the eligibility sections of this COC).
180 2024 UMP CDHP (PEBB) Certificate of Coverage
Medical benefit
Medical benefit refers to services subject to your deductible and coinsurance. See the “What you pay for
services” section for a description of how this works.
Medical emergency
A medical emergency means a medical condition that manifests itself by acute symptoms of sufficient
severity (including severe pain) so that a prudent layperson who has an average knowledge of medicine
and health would reasonably expect that not seeking immediate medical treatment at an emergency
room would result in any one of the following:
• Places the member’s health, or with respect to pregnancy, the health of an unborn child, in serious
jeopardy;
• Causes serious impairment to bodily functions; or
• Causes serious dysfunction of any bodily organ or part.
Medical food
Medical food is food administered under the supervision of a provider, intended for the specific dietary
management of a disease or condition for which there are distinctive nutritional requirements.
Medically necessary or medical necessity
ALERT! The provider or member must provide documentation demonstrating medical
necessity when requested by the plan, or the plan may deny services as not medically
necessary. The plan may not cover some medically necessary services. All benefits or services
that are medically necessary are subject to the plan’s coverage limitations, exclusions, and
provisions of the plan. It is important to review this COC or verify coverage with UMP Customer
Service before receiving services.
Medically necessary or medical necessity means health care services, supplies, prescription drugs, or
interventions that a licensed health care provider recommends and all the following conditions are met:
• The purpose of the service, supply, intervention, or prescription drug is to prevent, evaluate, treat, or
diagnose an illness, injury, disease, or its symptoms.
• The level of service, supply, intervention, prescription drug, or prescription drug dose is appropriate
considering the potential benefits and harm to the member.
• The level of service, supply, intervention, prescription drug, or prescription drug dose is known to be
effective in improving health outcomes.
• The level of service, supply, intervention, prescription drug, or prescription drug dose recommended for
this condition is cost-effective compared to alternative interventions, including no intervention.
• The service, supply, or intervention is not being recommended for reasons of convenience to the
patient or health care provider.
• For services that the HTCC has reviewed, and that UMP has implemented, medical necessity is
established only when HTCC’s coverage conditions are met.
2024 UMP CDHP (PEBB) Certificate of Coverage 181
The fact that a physician or other provider prescribes, orders, recommends, or approves a service or
supply, prescription drug, or prescription drug dose does not make it medically necessary.
The plan may require proof that services, interventions, supplies, or prescription drugs (including court-
ordered care) are medically necessary. Depending on the circumstances, such proof may be
documentation about the member’s condition or scientific evidence about the effectiveness of the
treatment.
The plan will not provide benefits if the required proof is not received, or does not adequately justify the
medical necessity of the service, supply, prescription drug, or prescription drug dose. Claims processing
may be delayed if proof of medical necessity is required but not adequately provided by the health
service provider.
The plan uses scientific evidence from peer-reviewed medical literature to determine effectiveness for
services and interventions not yet in widespread use for the medical condition and member indications
being considered.
For services that the HTCC has reviewed, and that UMP has implemented, state law requires that UMP use
the HTCC’s coverage criteria in determining whether the service is medically necessary. When the HTCC
determines that a service is not covered, then the service is not covered by the plan. If the HTCC
determines that a service is covered, then the HTCC’s criteria (if any) determine medical necessity. The
HTCC’s decisions and related documentation are available on the HCA website at hca.wa.gov/hta.
For services, interventions, supplies, prescription drugs, or prescription drug doses not related to an HTCC
review, the plan first uses scientific evidence, then professional standards, then expert opinion to
determine coverage.
Scientific evidence consists primarily of controlled clinical trials that either directly or indirectly
demonstrate the effect of the intervention on health outcomes. If controlled clinical trials are not available,
observational studies that demonstrate a causal relationship between the intervention and health
outcomes may be used. Partially controlled observational studies and uncontrolled clinical series may be
suggestive, but do not by themselves demonstrate a causal relationship unless the magnitude of the
effect observed exceeds anything that could be explained either by the natural history of the medical
condition or potential experimental biases.
Interventions for which clinical trials have not been conducted because of epidemiological reasons (that is,
rare or new diseases or orphan populations) shall be evaluated based on professional standards of care or
expert opinion.
A level of service, supply, prescription drug, prescription drug dose, or intervention is considered cost
effective if the benefits and harms relative to the costs represent an economically efficient use of
resources for members with this condition. The plan applies this criterion based on the individual
member’s medical situation and characteristics. Cost-effective does not always mean the lowest price.
Preventive services not covered by the plan’s preventive care benefit will still be covered under the
medical benefit or prescription drug benefit if the outlined criteria are met for medical necessity.
Member
A member is an eligible employee, retiree, former employee or former dependent in Continuation
Coverage, survivor, or dependent enrolled in the plan (see also the “Enrollee” definition).
Necessary contact lenses
Necessary contact lenses are contact lenses that are prescribed by your provider for other than elective
or cosmetic purposes. Necessary contact lenses are used to treat specific conditions for which contact
lenses provide better visual correction.
182 2024 UMP CDHP (PEBB) Certificate of Coverage
Network
Network is the preferred and participating facilities, providers, and suppliers your health plan contracts
with to provide health care services.
Network pharmacy
A network pharmacy contracts with WSRxS to provide prescription drug coverage to UMP members at the
contracted rate (allowed amount). See the “Where to buy your prescription drugs” section for details
about the advantages of using network pharmacies.
Network provider
A network provider is a preferred or participating provider. See the “Participating provider” definition
and the “Preferred provider” definition for specific details.
Network rate
The network rate means the plan pays 85 percent of the allowed amount for preferred providers after
you meet your medical deductible.
Network status
Network status refers to whether a provider is preferred, participating, or out-of-network with the plan.
You may find out the network status of your provider by visiting the UMP Provider search or by
contacting UMP Customer Service (see Directory for link and contact information).
Network vaccination pharmacy
A network vaccination pharmacy is a pharmacy that contracts with WSRxS to give covered
immunizations to plan members at the preventive rate. You may find out which pharmacies are contracted
on the UMP Prescription drug coverage webpage or by contacting WSRxS Customer Service (see
Directory for link and contact information).
Noncovered prescription drugs
Noncovered prescription drugs refer to any drug that is only covered if the member receives an
exception from the plan. Some drugs may be medically necessary, yet still are not covered. See the
"Prescription drugs and products UMP does not cover" section.
Noncovered services
Noncovered services refers to any medical service that is not covered by the plan. Some services may be
medically necessary, yet still are not covered. See the “What the plan does not cover” section. When the
HTCC determines that a service is not covered, then the service is not covered by the plan.
Nonduplication of benefits
Nonduplication of benefits is how UMP coordinates benefits when UMP is your secondary coverage.
When another plan is primary (pays first), that plan pays their normal benefit. UMP then pays up to the
amount we would have paid if UMP had been the primary plan. If the primary plan pays as much or more
than the normal UMP benefit, UMP pays nothing. UMP does not pay the rest of the allowed amount. See
examples on page 119.
2024 UMP CDHP (PEBB) Certificate of Coverage 183
Non-network pharmacy
A non-network pharmacy does not contract with WSRxS. See page 96 for what happens if you use a
non-network pharmacy to purchase covered prescription drugs. Non-network pharmacies do not include
excluded pharmacies (see the definition of “Excluded pharmacy”).
Nonprescription alternative
A nonprescription alternative includes an over-the-counter drug, dietary supplement, herbal
supplement, vitamin, mineral, medical food, or medical device that you may buy without a prescription
that has similar safety, efficacy, and ingredients as a prescription drug.
Nonprescription drug
A nonprescription drug includes an over-the-counter drug, dietary supplement, herbal supplement,
vitamin, mineral, medical food, or medical device that you may buy without a prescription.
Normal benefit
The plan’s normal benefit is the dollar amount the plan would normally pay if no other group health plan
had the primary responsibility to pay the claim for a benefit.
Occupational injury or illness
An occupational injury or illness is one resulting from work that is for pay or profit.
Orthognathic and Telegnathic surgery
Orthognathic surgery is surgery to correct conditions of the jaw and face related to structure, growth, or
TMJ disorders, or to correct orthodontic problems that cannot be easily treated with braces.
Telegnathic surgery means skeletal advancement to enlarge and stabilize the pharyngeal airway to treat
obstructive sleep apnea.
Out-of-network provider(s)
An out-of-network provider is a health care provider that is:
• In the Regence BlueShield service area, but is not contracted as part of Regence BlueShield’s PPO
network; or
• Outside the Regence BlueShield service area but is not contracted with another Blue Cross or Blue
Shield organization in the BlueCard® Program (designated as a provider in the PPO network) to
provide services and supplies to plan members.
See page 17 for a description of how services by these providers are covered.
Out-of-network provider(s), vision
Out-of-network provider(s), vision do not have a contract with VSP.
Out-of-network rate
Out-of-network providers are paid at the out-of-network rate. When you receive medical services from
out-of-network providers, you pay 40 percent of the allowed amount after you meet your deductible. You
pay all charges billed to you above the allowed amount (known as balance billing). The plan pays 60
percent of the allowed amount.
184 2024 UMP CDHP (PEBB) Certificate of Coverage
Out-of-pocket limit
The out-of-pocket limit is the most you pay during a calendar year for covered medical services and
prescription drugs before the plan pays 100 percent of the allowed amount to preferred providers and
network pharmacies. This limit does not include your premium, balance-billed charges, or services the
plan does not cover.
For this plan, the limit is $4,200 for one member enrolled in the plan, or $8,400 if there are two or more
members enrolled in the plan. However, no one member may exceed $7,000 in covered out-of-pocket
expenses annually. Once the out-of-pocket limit has been reached, the plan pays 100 percent of the
allowed amount for covered medical services from preferred providers and 100 percent of the allowed
amount for covered prescription drugs and products for the rest of the calendar year.
See page 28 for what does and does not apply to this limit. Your deductible does apply to this limit.
Outpatient rate
The plan’s outpatient rate depends on the provider’s status:
• Preferred providers: You pay 15 percent of the allowed amount after you meet your deductible. The
plan pays 85 percent of the allowed amount.
• Participating providers: You pay 40 percent of the allowed amount after you meet your deductible. The
plan pays 60 percent of the allowed amount.
• Out-of-network providers: You pay 40 percent of the allowed amount after you meet your deductible.
You pay all charges billed to you above the allowed amount (known as balance billing). The plan pays
60 percent of the allowed amount.
Outpatient surgery center
See the “Ambulatory surgery center (ASC)” definition.
Outward Bound
An international network of outdoor education organizations whose aim is to foster the personal growth
and social skills of participants by using challenging expeditions in the outdoors.
Over-the-counter alternative
An over-the-counter alternative is a drug that you may buy without a prescription that has similar
safety, efficacy, and ingredients as a prescription drug.
Over-the-counter drugs
Over-the-counter drugs are medications you may get without a prescription.
Over-the-counter equivalent
An over-the-counter equivalent is a drug you may buy without a prescription that has identical active
ingredients and strengths as a prescription drug or product in a comparable dosage form.
P&T Committee
See the “Pharmacy & Therapeutics (P&T) Committee” definition.
2024 UMP CDHP (PEBB) Certificate of Coverage 185
Partial Hospitalization Program
Partial Hospitalization Program (PHP) is an outpatient program that is provided under the supervision
of an attending psychiatrist or psychiatric extender. PHP is intended to provide treatment on an
outpatient basis, does not include boarding or housing, and is intended to provide treatment
interventions in a structured setting, with patients returning to their home environments each day. PHP is
a minimum of five hours per day, five days per week.
Participating provider
A participating provider is:
• Contracted with Regence BlueShield but is not in your plan’s preferred network, and they cannot
balance bill you.
• Considered out of network for your plan, except for the following services:
▪ Covered preventive services.
▪ Mental health or substance use disorder.
▪ Emergency services for a medical emergency (including air ambulance).
Peer-reviewed medical literature
Peer-reviewed medical literature is scientific studies printed in journals or other publications in which
original manuscripts are published only after being critically reviewed for scientific accuracy, validity, and
reliability by unbiased independent experts. Peer-reviewed medical literature, for example, does not
include information from health-related websites or in-house publications of pharmaceutical
manufacturers.
Pharmacy & Therapeutics (P&T) Committee
Pharmacy & Therapeutics (P&T) Committee is a group of providers and other health care professionals
who review prescription drugs and make recommendations on the status of prescription drugs on the
UMP Preferred Drug List (see “The UMP Preferred Drug List” section for more information).
Physician services
Physician services are health care services provided or coordinated by a licensed medical physician, such
as a:
• Doctor of osteopathic medicine (D.O.)
• Medical doctor (M.D.)
• Naturopathic physician (N.D.)
Find the complete list of covered provider types on the UMP website at
ump.regence.com/pebb/benefits/providers/covered-providers.
Plan
Plan, as referred to in this document, means Uniform Medical Plan Consumer-directed Health Plan (UMP
CDHP), a self-insured PPO plan offered by the PEBB Program. In the eligibility sections (see “Eligibility for
subscribers and dependents on page 140 or 155), “plan” may include other plans not sponsored by the
PEBB Program. In the “If you have other HDHP coverage” section, “plan” may mean any health insurance
coverage.
186 2024 UMP CDHP (PEBB) Certificate of Coverage
Preauthorization
Preauthorization is plan approval for coverage of specific services, supplies, or prescription drugs before
they are provided to the member. Preauthorization is not a guarantee of coverage. If you or your provider
do not receive preauthorization for certain medical services or prescription drugs, the plan may deny the
claim. See the “Preauthorizing medical services” section for how this works. A list of medical services that
require preauthorization is available on the UMP Policies that affect your care webpage or by contacting
UMP Customer Service (see Directory for link and contact information). See page 98 for information on
prescription drugs that must be preauthorized.
Preferred drug
A preferred drug is a prescription drug that is listed on the UMP Preferred Drug List.
Preferred Drug List
The UMP Preferred Drug List is a list available online that specifies how prescription drugs are covered
by the plan. By using this list, you may find out if a prescription drug is covered, how much you will pay, if
the drug must be ordered through the plan’s specialty drug pharmacy, and whether the drug has any
limitations (such as needing preauthorization or quantity limits; see the ”Limits on your prescription drug
coverage” section).
The UMP Preferred Drug List is based on the Washington Preferred Drug List and recommendations by
one of the P&T Committees that partner with WSRxS (see the “How UMP decides which prescription
drugs are preferred” section for more information).
Preferred provider(s)
A preferred provider is a provider:
• In the Regence service area and contracted as part of Regence BlueShield’s PPO network; or
• Outside the Regence service area and contracted with another Blue Cross or Blue Shield organization in
the BlueCard® Program (designated as a Provider in the “Preferred Provider Organization (“PPO”)
Network”) to provide services and supplies to plan members.
Preferred Provider Organization (PPO)
A Preferred Provider Organization (PPO) is a health plan that has a network of providers who have
agreed to provide services at discounted rates. Members may self-refer to most specialists. UMP CDHP is
a PPO.
Prenatal
Prenatal means during pregnancy.
Prescription drug
Prescription drug means a drug approved by the FDA that can be dispensed only with an order given by
a properly authorized person. The designation of a medication as a prescription drug is made by the FDA.
Preventive care
Preventive care means those services described by the Public Health Services Act, Section 2713:
• Covered immunizations recommended by the CDC.
2024 UMP CDHP (PEBB) Certificate of Coverage 187
• Evidence-informed preventive care and screenings for women as described in HRSA Guidelines in
accordance with 45 CFR §147.130 (a)(iv).
• Evidence-informed preventive care screenings for infants, children, and adolescents supported by the
Health Resources and Services Administration (HRSA).
• Services with an A or B rating by the U.S. Preventive Services Task Force.
Preventive rate
Covered preventive services are not subject to your deductible. The plan’s preventive rate depends on
the provider’s status:
• Preferred providers: You pay $0. The plan pays 100 percent of the allowed amount.
• Participating providers: You pay $0. The plan pays 100 percent of the allowed amount.
• Out-of-network providers: You pay 40 percent of the allowed amount. You pay all charges billed to you
above the allowed amount (known as balance billing). The plan pays 60 percent of the allowed amount.
Primary care provider (PCP)
A primary care provider (PCP) is a physician (see the “Physician services” definition), nurse practitioner,
or physician assistant who provides, coordinates, or helps a member access a range of health care
services. See page 19 for a list of specialties that may be a primary care provider.
Primary payer
The primary payer is the insurance plan that processes the claim first when a member has more than one
group insurance plan covering the services and the plans must coordinate benefits.
Professional services
Professional services are non-facility medical services performed by professional providers, including,
but not limited to, medical doctors, doctors of osteopathy, naturopathic physicians, and advanced
registered nurse practitioners.
Provider
A provider is an individual medical professional (such as a doctor or nurse), hospital, skilled nursing
facility, pharmacy, program, equipment and supply vendor, or other facility, organization, or entity that
provides care or bills for health care services or products.
Provider network
A provider network is a group of providers who negotiate a contract with Regence BlueShield to provide
health care services to plan members. These providers have agreed to see members under certain rules,
including billing at contracted rates (see the “Allowed amount, medical services” definition). The Regence
BlueShield, including the BlueCard Program, provider network for UMP CDHP members in 2024 consist of
preferred and participating providers.
Public Employees Benefits Board (PEBB)
The Public Employees Benefits Board (PEBB), is a group of representatives, appointed by the governor,
who approves insurance benefit plans for employees and their dependents, and establishes eligibility
criteria for participation in insurance benefit plans.
188 2024 UMP CDHP (PEBB) Certificate of Coverage
Public Employees Benefits Board (PEBB) plan
A Public Employees Benefits Board (PEBB) plan is one of several health benefit plans, including the
Uniform Medical Plan (UMP Classic, UMP Select, UMP Consumer-Directed Health Plan, and UMP Plus
plans: UMP Plus–Puget Sound High Value Network and UMP Plus–UW Medicine Accountable Care
Network), offered through the PEBB Program to eligible public employees, former employees and
dependents in Continuation Coverage, retirees, survivors, retired employees of a former employer group,
and their eligible dependents. The PEB Board designs benefits and eligibility and is administered by HCA
as part of a comprehensive benefits package.
Public Employees Benefits Board (PEBB) Program
The Public Employees Benefits Board (PEBB) Program is the HCA program that administers PEBB
benefit eligibility and enrollment.
Qualified medical expense
A qualified medical expense is a cost payable through an HSA, without paying income tax or tax
penalties. See IRS publication 502 for the complete definition. IRS publication 502 also lists the specific
types of services and supplies that qualify. You may also access a list on the HealthEquity website (see
Directory for link).
Quantity limit
A quantity limit is a limit on how much of a prescription drug you may get for a specific time period
(days’ supply).
Reconstructive surgery
Reconstructive surgery is surgery and follow-up treatment needed to correct or improve a part of the
body because of birth defects, accidents, injuries, or medical conditions.
Regence BlueShield service area
The Regence BlueShield service area means the Washington counties of Clallam, Columbia, Cowlitz,
Grays Harbor, Jefferson, King, Kitsap, Klickitat, Lewis, Mason, Pacific, Pierce, San Juan, Skagit, Skamania,
Snohomish, Thurston, Yakima, Wahkiakum, Walla Walla, Whatcom, and any other areas designated by
Regence. Check the Regence website at regence.com for up-to-date information.
Rehabilitative services
Rehabilitative services are health care services that help you keep, get back, or improve skills and
functioning for daily living that have been lost or impaired because you were sick, hurt, or disabled. These
services may include physical and occupational therapy, speech-language pathology, and psychiatric
rehabilitation services in a variety of inpatient and/or outpatient settings.
Residential treatment facility
Residential treatment facility means a facility that offers a defined course of therapeutic intervention
and special programming in a controlled environment; offers a degree of security, supervision, and
structure; and is licensed by the appropriate state and local authority to provide such services. Patients
also must be medically monitored with 24-hour medical availability and 24-hour onsite clinician services.
Residential treatment facilities typically do not include halfway houses; supervised living; group homes;
wilderness courses or camps; Outward Bound; outdoor youth programs; boarding houses; or settings that
2024 UMP CDHP (PEBB) Certificate of Coverage 189
primarily either focus on building self-esteem or leadership skills or provide a supportive environment to
address long-term social needs. However, services by providers in such settings may be covered if they
are billed separately and otherwise would be covered.
Respite care
Respite care is continuous care for a homebound hospice member of more than four hours a day to
provide family members temporary relief from caring for the member.
Retired employee of a former employer group
A retired employee of a former employer group includes a retired employee from a PEBB employer
group and a retired school employee of a SEBB employer group who is continuing enrollment in PEBB
health plan coverage by self-paying premiums after losing eligibility for PEBB retiree insurance coverage
upon the employer group ending participation in insurance plans and contracts with the health care
authority (HCA).
Routine
Routine services are those provided as preventive, not because of an injury or illness. In the case of
covered immunizations, routine refers to covered immunizations included on the CDC schedules (see
page 67).
Same-day surgery center
See the “Ambulatory surgery center (ASC)” definition.
School Employees Benefits Board (SEBB)
The School Employees Benefits Board (SEBB) is a group of representatives, appointed by the governor,
who designs and approves insurance benefit plans for school employees and their dependents, and
establishes eligibility criteria for participation in insurance benefit plans.
School Employees Benefits Board (SEBB) Program
The School Employees Benefits Board (SEBB) Program is the program within HCA that administers
insurance and other benefits for eligible school employees and eligible dependents.
Scientific evidence
Scientific evidence means scientific studies published in or accepted for publication by medical journals
that meet nationally recognized requirements for scientific manuscripts and that submit most of their
published articles for review by experts who are not part of the editorial staff. Scientific evidence also
refers to findings, studies, or research conducted by or under the auspices of federal government
agencies and nationally recognized federal research institutes. However, scientific evidence does not
include published peer-reviewed literature sponsored to a significant extent by a pharmaceutical
manufacturing company or medical device manufacturer or a single study without other supportable
studies.
Scope of practice
Scope of practice refers to the services a provider may perform and bill for, based on the provider’s
professional license as issued by local authorities. For example, some provider types may prescribe
prescription drugs, and some may not.
190 2024 UMP CDHP (PEBB) Certificate of Coverage
Screening
Screening refers to services performed to prevent or detect illness in the absence of disease or
symptoms.
Secondary coverage
When you are covered by more than one group health plan, you have secondary coverage that may pay
a part or the rest of a provider’s bill after your primary payer has paid. See the “If you have other HDHP
coverage” section for more information on how this plan coordinates benefits.
Skilled nursing care
Skilled nursing care is services from licensed nurses in your own home or in a nursing home. Skilled care
services are from technicians and therapists in your own home or in a nursing home.
Skilled nursing facility
A skilled nursing facility is an institution, or part of an institution, that provides skilled nursing care 24
hours a day and is classified as a skilled nursing facility by Medicare. Medicaid-eligible, long-term care
facilities are not necessarily skilled nursing facilities.
SmartHealth
SmartHealth is a voluntary wellness program offered by the PEBB Program that allows eligible
subscribers to earn wellness incentives.
Employees who waive medical and eligible retirees who defer PEBB retiree insurance coverage are not
eligible to qualify for the incentive. The wellness incentive that you qualify for during the 2023 plan year is
deposited into your HSA in January 2024 if you are still eligible to participate in the wellness incentive
program. The wellness incentive that you qualify for during the 2024 plan year is deposited into your HSA
in January 2025 if you are still eligible to participate in the wellness incentive program and are enrolled in
the 2025 plan year. The wellness incentive applies to your maximum annual contribution limit.
More details on eligibility and program requirements are on HCA's SmartHealth webpage at
hca.wa.gov/pebb-smarthealth.
Special rate
The plan’s special rate is for services that have unique payment rules. These rules are described in the
table (see the “How much you pay for covered services” column) located in the “Types of services” section.
Specialty drugs
Specialty drugs are high-cost injectable, infused, oral, or inhaled prescription drugs or products that
require special storage or handling and are subject to additional rules. Specialty drugs are identified on
the UMP Preferred Drug List. See page 99 for information on how specialty drug prescriptions are
handled.
Standard rate
The plan’s standard rate depends on the provider’s status:
• Preferred providers: You pay 15 percent of the allowed amount after you meet your deductible. The
plan pays 85 percent of the allowed amount.
2024 UMP CDHP (PEBB) Certificate of Coverage 191
• Participating providers: You pay 40 percent of the allowed amount after you meet your deductible. The
plan pays 60 percent of the allowed amount.
• Out-of-network providers: You pay 40 percent of the allowed amount after you meet your deductible.
You pay all charges billed to you above the allowed amount (known as balance billing). The plan pays
60 percent of the allowed amount.
Standard reference compendium
Standard reference compendium refers to any of these sources:
• The American Hospital Formulary Service Drug Information
• The American Medical Association Drug Evaluation
• The United States Pharmacopoeia Drug Information
• Other authoritative compendia as identified from time to time by the U.S. Secretary of Health and
Human Services
State Agency
State agency means an office, department, board, commission, institution, or other separate unit or
division, however designated, of the Washington state government. It includes the legislature, executive
branch, and agencies or courts within the judicial branch, as well as institutions of higher education and
any unit of state government established by law.
State-registered domestic partner
State-registered domestic partner means an adult who meets the requirements for a valid state-
registered domestic partnership and has been issued a certificate of state-registered domestic partnership
by the Washington State Secretary of State, or an adult whose legal union (other than a marriage) was
validly formed in another jurisdiction and is substantially equivalent to a domestic partnership under
Washington law.
Subscriber
A subscriber is an eligible employee, retiree, former employee or former dependent in Continuation
Coverage, retired employee of a former employer group, or survivor who is the primary certificate holder
and plan member.
Substance use disorder
Substance use disorder is an illness characterized by a physiological or psychological dependency on a
controlled substance or alcohol.
Substance use disorder facility
A substance use disorder facility is an institution, or part of an institution, that specifically treats
dependency on a controlled substance or alcohol and meets all of these criteria:
• Is certified by the Washington State Division of Behavioral Health and Recovery (DBHR), or for facilities
outside of the Regence BlueShield service area, is contracted with the local BlueCard® network
• Is licensed by the state
• Keeps adequate patient records that contain course of treatment, progress, discharge summary, and
follow-up programs
192 2024 UMP CDHP (PEBB) Certificate of Coverage
• Performs services under full-time supervision of a physician or registered nurse
• Provides services, for a fee, to persons receiving substance use disorder treatment, including room and
board, as well as 24-hour nursing
Therapeutic alternative
A therapeutic alternative is a drug that is not chemically identical to a nonpreferred drug but has similar
effects when given in therapeutically equivalent doses.
Therapeutic equivalent
A therapeutic equivalent is a drug that is chemically identical to a nonpreferred drug and is expected to
have the same effectiveness and toxicity when given in the same doses.
Therapeutic interchange
Therapeutic interchange is when a pharmacist, with the endorsing provider’s permission (see page 101),
substitutes a nonpreferred prescription drug with a preferred drug that is a therapeutic alternative or
equivalent.
Tobacco cessation services
Tobacco cessation services are provided for quitting tobacco use through counseling and nicotine
replacement therapy products.
Unicompartmental
Unicompartmental refers to a diagnosis or procedure affecting only one part, or “component,” of a joint
(e.g. knee) as opposed to more than one part of a joint.
Uniform Medical Plan Consumer-directed Health Plan (UMP
CDHP)
Uniform Medical Plan Consumer-directed Health Plan (UMP CDHP) is a self-insured PPO health plan
offered through the PEBB Program and managed by HCA.
VSP Choice network provider, vision
VSP Choice network provider, vision means an optometrist or ophthalmologist licensed and otherwise
qualified to practice vision care and/or provide vision care materials who has contracted with VSP to
provide vision care services and/or vision care materials to members. This plan’s provider network is VSP
Choice.
Disclosures
If you need this document in another format or if you need information about how to file a discrimination
complaint, read the UMP nondiscrimination and language assistance notice by visiting hca.wa.gov/ump-
nondiscrimination.
Advice24, Ardon Health, CoverMyMeds, Moda Health, Postal Prescription Services (PPS), Costco Mail-
Order Pharmacy, Washington State Rx Services (WSRxS), Premera Blue Cross, and SmartHealth do not
provide Blue Cross Blue Shield services and are separate companies solely responsible for their
products.VSP is a separate company that provides vision services.

2024 UMP CDHP (PEBB) Certificate of Coverage 193
HealthEquity is a separate company that provides health savings account administration services.
Doctor on Demand is a separate company that provides telehealth services.
Quartet is a separate company that provides assistance accessing behavioral health services.
Omada Health is a separate company that provides diabetes prevention program.
2nd.MD is a separate company that provides treatment decision support through their Expert Second
Opinion program.
myStrength is a separate company that provides virtual behavioral health care services.
